
Occult Hernia
What are Occult Hernias?
- Light, D., Ratnasingham, K., Banerjee, A., Cadwallader, R., Uzzaman, M. M., & Gopinath, B. (2011). The role of ultrasound scan in the diagnosis of occult inguinal hernias. International Journal of Surgery, 9(2), 169-172. Retrieved from https://www.sciencedirect.com/science/article/pii/S1743919110004784#:~:text=Introduction,differentiate%20it%20from%20other%20causes.
“Very small inguinal hernias which are difficult to diagnose on clinical examination are defined as ‘occult inguinal hernias’”.
- Miller, J., Cho, J., Michael, M. J., Saouaf, R., & Towfigh, S. (2014). Role of imaging in the diagnosis of occult hernias. JAMA surgery, 149(10), 1077-1080. Retrieved from https://jamanetwork.com/journals/jamasurgery/fullarticle/1893806
“Hidden hernias are nonpalpable hernias, more commonly seen among women. The primary symptom is pain, without a noticeable bulge. Ultrasonography and CT do not reliably detect hidden hernias. Patients with clinical suspicion of an inguinal hernia should undergo imaging, with MRI as the most sensitive radiologic examination. If results of US or a CT scan are negative for inguinal hernia, then MRI should be performed to definitively rule out hernias.”
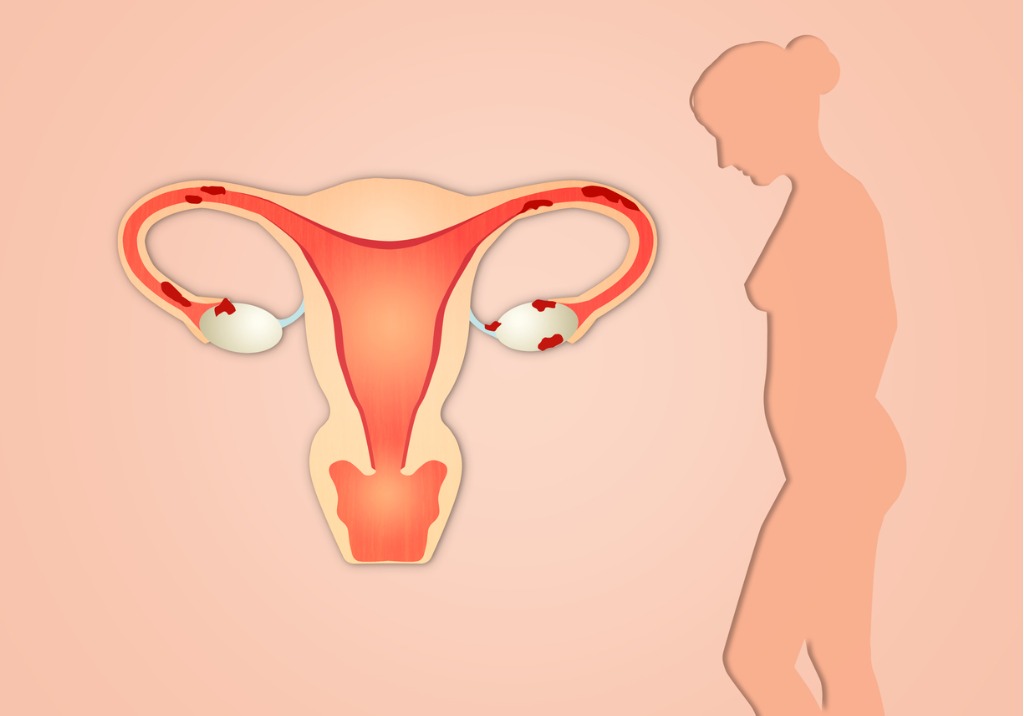
Endometriosis and Occult Hernia
- Sarrel, S. (2019). 2405 The Cult of the Occult Hernia and the Endometriosis Population. Journal of Minimally Invasive Gynecology, 26(7), S188. Retrieved from https://www.sciencedirect.com/science/article/pii/S1553465019307745
“Occult hernia may contribute to pain during sex, genital pain, groin pain, pelvic floor pain, increased lower abdominal pain during menstruation, perceived urinary pressure and leg pain. In the patient with endometriosis hernia may be missed during follow-up visits and surgery with the gynecologist. As a driver in pelvic pain, occult hernia should become more widely recognized as a source of pelvic pain.”
Pelvic Congestion Syndrome
Pelvic Congestion Syndrome- another cause of chronic pelvic pain
When talking about endometriosis and chronic pelvic pain, it is important to remember that often endometriosis is not the only pelvic pain generator. Another possible contributor to chronic pelvic pain is pelvic congestion syndrome (PCS). PCS is like having varicose veins in the pelvis. Blood pulls in the veins and can cause symptoms such as heaviness, pain with penetration, noncyclical pain, positional lower back pain, pelvic and upper thigh pain, prolonged postcoital discomfort, symptoms that worsen throughout the day and are exacerbated by activity or prolonged standing, and non-specific lower abdominal and pelvic pain (Durham & Machan, 2013; Mistry & le Roux, 2017). LIANG and Brown (2021) report that:
“Typical pelvic congestion syndrome pain is:
– Heaviness and dull aching in nature
– Located deep in the pelvis and on the left
– Exacerbated by upright position (standing or sitting) and exercise (walking, running, weightlifting)
– Worse towards the end of the day
– Worse after sexual intercourse
– Worse when bladder is full
– Chronic and insidious onset
Atypical pelvic congestion syndrome pain is:
– Constant pain not related to time of day, upright posture or physical activities
– Pain worse premenstrually and during menstrual periods
– More on the right than the left
– Acute and sudden onset
– Sharp or colicky in nature”
While the gold standard for diagnosis is contrast venogram, this procedure is usually done as part of the treatment (embolization procedure) (LIANG & Brown, 2021). LIANG and Brown (2021) report that “all non-invasive imaging like ultrasound, CT and MRI can detect pelvic varicosities” but that the key is “to alert the imaging technicians and specialist to look out for pelvic varicosities and to report them” (LIANG & Brown, 2021). A CT scan can also help diagnose other syndromes such as Nutcracker Syndrome (left renal vein compression) and May-Thurner Syndrome (left iliac vein compression) (LIANG & Brown, 2021). If you’ve had surgeries before for endometriosis and wonder why it wasn’t seen during surgery, it is because surgery “is performed with the patient in supine or Trendelenburg position, and with the use of CO2 for abdominal distention” thus meaning that the “veins are often collapsed, and pelvic varicosities can be missed”- it would take the surgeon who suspects pelvic varicosities to put the patient in “reverse Trendelenburg position and easing off CO2 distention” that “might allow the dilated veins to fill” and possibly be seen (LIANG & Brown, 2021).
Unfortunately, PCS doesn’t just go away or improve with time, therefore, treatment is usually needed for those who are symptomatic (LIANG & Brown, 2021). Because there is pooling and back flow of blood in the veins, the treatment suggested is transcatheter embolization (LIANG & Brown, 2021). Medication, hysterectomy, and other treatments have not proved as effective (LIANG & Brown, 2021). The transcatheter embolization “is performed with conscious sedation under local anaesthetic, as a day procedure” and “is one of the safest embolisation procedures” (LIANG & Brown, 2021). LIANG and Brown (2021) report that “some feel the relief of pelvic congestion syndrome symptoms soon after embolisation, while others might have to wait for the thrombophlebitis to settle before appreciating the result”- reporting that it is best to wait 4-6 weeks to better judge the effectiveness. Mistry & le Roux (2017) report that after looking at 20 studies that “the overall technical success rate was as high as 99%” and that “with a mean follow up of 15 months, 80% of the patients reported benefit from the procedure while 13% experienced little or no relief of the symptoms”.
PCS may be another piece in the puzzle of ongoing chronic pelvic pain.
References
Durham, J. D., & Machan, L. (2013, December). Pelvic congestion syndrome. In Seminars in interventional radiology (Vol. 30, No. 04, pp. 372-380). Thieme Medical Publishers. Retrieved from https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0033-1359731
LIANG, D. E., & Brown, B. (2021). Pelvic congestion syndrome: Are we missing the diagnosis?. The Medical Republic. Retrieved from https://www.sydneyfibroidclinic.com.au/app/uploads/2021/06/PCS-Medical-Republic.pdf
Mistry, P. P., & le Roux, D. A. (2017). Pelvic congestion syndrome (PCS). Practice Perspectives for Venous Disorders, 46. Retrieved from http://www.vascularsociety.co.za/wp-content/uploads/2019/02/VASSA-venous-guidelines-Practice-perspectives-for-venous-disorders-2017.pdf#page=46
About Pelvic Congestion Syndrome:
- Durham, J. D., & Machan, L. (2013, December). Pelvic congestion syndrome. In Seminars in interventional radiology (Vol. 30, No. 04, pp. 372-380). Thieme Medical Publishers. Retrieved from https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0033-1359731
“Patients with pelvic congestion syndrome present with otherwise unexplained chronic pelvic pain that has been present for greater than 6 months, and anatomic findings that include pelvic venous insufficiency and pelvic varicosities. It remains an underdiagnosed explanation for pelvic pain in young, premenopausal, usually multiparous females. Symptoms include noncyclical, positional lower back, pelvic and upper thigh pain, dyspareunia, and prolonged postcoital discomfort. Symptoms worsen throughout the day and are exacerbated by activity or prolonged standing. Examination may reveal ovarian tenderness and unusual varicosities—vulvoperineal, posterior thigh, and gluteal. Diagnosis is suspected by clinical history and imaging that demonstrates pelvic varicosities. Venography is usually necessary to confirm ovarian vein reflux, although transvaginal ultrasound may be useful in documenting this finding. Endovascular therapy has been validated by several large patient series with long-term follow-up using standardized pain assessment surveys. Embolization has been shown to be significantly more effective than surgical therapy in improving symptoms in patients who fail hormonal therapy. Although there has been variation in approaches between investigators, the goal is elimination of ovarian vein reflux with or without direct sclerosis of enlarged pelvic varicosities. Symptom reduction is seen in 70 to 90% of the treated females despite technical variation.”
Links:
- Semmel, D. (2013). Which Options Are Best for Pelvic Congestion Syndrome?. Retrieved from https://www.empr.com/home/features/which-options-are-best-for-pelvic-congestion-syndrome/
Pudendal Neuralgia and Vulvodynia
Links:
Pudendal Neuralgia:
“Pudendal neuralgia is described as a neuropathic pain in the distribution of the pudendal nerve” (Hibner, Desai, Robertson, & Nour, 2010).
- Symptoms
- Pudendal Neuralgia Symptoms. https://www.pudendalhope.info/pudendal-neuralgia-symptoms/
“The main symptom of pudendal neuralgia (PN) and pudendal nerve entrapment (PNE) is pain in one or more of the areas innervated by the pudendal nerve or one of its branches. These areas include the rectum, anus, urethra, perineum, and genital area. In women this includes the clitoris, mons pubis, vulva, lower 1/3 of the vagina, and labia. In men this includes the penis and scrotum. But often pain is referred to nearby areas in the pelvis. The symptoms can start suddenly or develop slowly over time. Typically pain gets worse as the day progresses and is worse with sitting. The pain can be on one or both sides and in any of the areas innervated by the pudendal nerve, depending on which nerve fibers and which nerve branches are affected. The skin in these areas may be hypersensitive to touch or pressure (hyperesthesia or allodynia).
“Possible symptoms include burning, numbness, increased sensitivity, electric shock or stabbing pain, knife-like or aching pain, feeling of a lump or foreign body in the vagina or rectum, twisting or pinching, abnormal temperature sensations, hot poker sensation, constipation, pain and straining with bowel movements, straining or burning when urinating, painful intercourse, and sexual dysfunction – persistent genital arousal disorder (genital arousal without desire) or the opposite problem – loss of sensation.
“It is not uncommon for PN to be accompanied by musculoskeletal pain in other parts of the pelvis such as the sacroiliac joint, piriformis muscle, or coccyx. It is usually very difficult to distinguish between PN and pelvic floor dysfunction because they are frequently seen together. Some people refer to this condition as pelvic myoneuropathy which suggests both a neural and muscular component involving tense muscles in the pelvic floor.
“Other Possible Symptoms
- The chief symptom is pain in the area innervated by the pudendal nerves such that sitting becomes intolerable.
- The pain may be lessened when sitting on a toilet seat or a doughnut pillow as this lessens the pressure on the pudendal nerve. Most people simply have to avoid sitting because it is impossible to find a cushion that relieves pain in all areas.
- The pain is often not immediate but delayed and continuous and stays long after one has discontinued the activity that caused the pain (stop sitting, cycling, sex…).
- Often the pain is lower in the morning upon awakening and increases throughout the day.
- There may be extreme pain or tenderness along the course of the nerve when the nerve is pressed on via the vagina or rectum.
- Pain in perineum.
- Pain after orgasm.
- Loss of sensation with difficulty achieving orgasm.
- Strange feeling of uncomfortable arousal without sexual desire.
- Intolerance to tight pants or elastic bands around the legs.
- Friction and feeling of inflammation along the course of the nerve when walking for too long or running.
- Constant pain even with standing or lying down.
- Problem with urinary retention after urination. Need to push to empty bladder. Harder to detect the feeling of urine when passing through the urethra.
- Urethral burning with or after urination
- Feeling like the bladder is never empty or feeling the need to urinate even when the bladder is empty.
- Urinary frequency.
- Pain after bowel movement. Sometimes sufferers also report pain prior to and during the bowel movement.
- Painful muscles spasms of the pelvic floor after bowel movement.
- Constipation.
- Sexual problems. Men complain of a diminution of sensations. Pain after ejaculation is common. For women pain during and after intercourse is often reported.
- Scrotum/Testicular pain is possible. The testicle itself is innervated by another nerve however the difference in pain from scrotum/testicle can be hard to detect.
- Buttock sciatica and everything that goes with it: numbness, coldness, sizzling sensation in legs, feet, or buttock. This is more often due to a reaction of the surrounding muscles to the pain in the pelvic region. It could also be from “cross talk” of the nerves.
- Low back pain resulting from radiation of the pain.
- The symptoms can be unilateral or bilateral. If the entrapment is only on one side, the pain can also be reflected to the other side.
- Some people develop conditions such as complex regional pain syndrome and even post-traumatic stress disorder after prolonged or severe pain.”
Vulvodynia:
- National Vulvodynia Association. (n.d.). What is vulvodynia?. Retrieved from https://www.nva.org/what-is-vulvodynia/
“Vulvodynia, simply put, is chronic vulvar pain without an identifiable cause. The location, constancy and severity of the pain vary among sufferers. Some women experience pain in only one area of the vulva, while others experience pain in multiple areas. The most commonly reported symptom is burning, but women’s descriptions of the pain vary. One woman reported her pain felt like “acid being poured on my skin,” while another described it as “constant knife-like pain.”… For women with generalized vulvodynia (GV), pain occurs spontaneously and is relatively constant, but there can be some periods of symptom relief. Activities that apply pressure to the vulva, such as prolonged sitting or simply wearing pants, typically exacerbate symptoms. Some women experience pain in a specific area, e.g., only in the left labia or near the clitoris, while others experience pain in multiple areas, e.g., in the labia, vestibule, and clitoris. In the latter group, pain may also occur in the perineum and inner thighs, as demonstrated in the diagram on the right.”
- Symptoms:
- Medical News Today. (2017).Vulvodynia: What you need to know. Retrieved from http://www.medicalnewstoday.com/articles/189076.php
“Pain is the most notable symptom of vulvodynia, and can be characterized as a burning, stinging, irritation or sharp pain that occurs in the vulva, including the labia and entrance to the vagina. It may be constant, intermittent or happening only when the vulva is touched, but vulvodynia is usually defined as lasting for at least three months. The pain is usually found around the urethra and at the top of the legs and inner thighs, and it can be either intermittent or constant. Symptoms may occur in one place or the entire vulvar area.
“The pain is usually described as a burning, stinging, itching, irritating or a raw feeling. Sexual intercourse, walking, sitting or exercising can make the pain worse. It can be present in the labia majora and/or labia minora. Sometimes it affects the clitoris, perineum, mons pubis and/or inner thighs. The pain may be constant or intermittent, and it is not necessarily initiated by touch or pressure to the vulva. The vulvar tissue may appear inflamed, but in most cases there are no visible findings. Vulvodynia usually starts suddenly and may last for months to years. Although it isn’t life-threatening, the pain may make one cut back on some normal activities. It can also make one upset or depressed. It might even cause problems in one’s relationship with spouse or partner, because it can make sexual intercourse painful.”
- Diagnosis:
- Fox, S. (2012). Vulvodynia and Interstitial Cystitis: Causes of Pelvic Pain; An Expert Interview With Susan Hoffstetter, PhD, WHNP-BC. Retrieved from https://www.medscape.com/viewarticle/773575#vp_2
“The best tool for making a diagnosis of vulvodynia is your ears — listen to what your patient is telling you! As part of the patient’s medical history, make sure you note any association between the onset or exacerbation of symptoms and life changes/stressors, changes in medical status, surgeries, and hormonal changes, including childbirth, lactation, and menopause. Physical examination should include evaluation for infection, inflammatory process, and vulvar dystrophies. Vulvodynia may present as generalized on the vulva or localized within the vestibule. Q-tip testing is very important in making the appropriate diagnosis of vulvodynia. Note if sensitivity is present on the vulva or within the vestibule at the Skene’s and Bartholin glands. Use a 0- to 10-point rating scale, with 0 being no pain/symptoms and 10 being the worst level of pain/symptoms. If a diagnosis of vulvodynia is made, Q-tip testing is helpful as an objective measure of level of discomfort (and hopefully improvement) over time. Vulvodynia is ultimately a diagnosis of exclusion after all other potential causes have been ruled out and symptoms have persisted for at least 6 month
- Treatment:
- Fox, S. (2012). Vulvodynia and interstitial cystitis: Causes of pelvic pain: An expert interview with Susan Hoffstetter, PhD, WHNP-BC. Retrieved from http://www.medscape.com/viewarticle/773575#2
“The initial treatment for any woman presenting with vulvar symptoms is to institute vulvar skin-care guidelines. These are designed to remove any contact irritants to the vulva, such as scented soaps, detergents, hot water, shaving, and washcloths. Neuropathic pain medications are the mainstay of treatment for vulvodynia. These alter the perception of pain by blocking reuptake transmitters, norepinephrine, and serotonin.
My first-line therapy is normally the tricyclic antidepressants, including amitriptyline, nortriptyline, and desipramine. I use amitriptyline primarily, which has a 60% response rate. It is generic and readily available at minimal cost. Fatigue is the primary side effect at the low doses used for treatment. Most patients develop a tolerance for this over time.
My next line of treatment is the anticonvulsants. Gabapentin can be used individually or in combination with amitriptyline. More than 60% of patients have shown significant improvement when prescribed gabapentin. I have also used pregabalin, which has been associated with results similar to gabapentin.
“Infrequently, I use amitriptyline 2% with baclofen 2% as a topical treatment, but that preparation must be compounded and has greater costs. If the patient has concurrent depression, I will also use a selective serotonin–norepinephrine reuptake inhibitor, such as duloxetine. I avoid most topical medications because they serve as a contact irritant over time and offer little symptom resolution. I have commonly seen women being prescribed topical lidocaine. This can become a contact irritant with routine use, but it can provide emergency relief to break the pain cycle.
“Many women with vulvodynia have increased resting tone, poor strength, and/or irritability of muscles. In those patients, biofeedback therapy can be very helpful. Biofeedback has a success rate of 60% to 80%. Physical therapy with a therapist trained in the pelvic-floor musculature can be very helpful, either alone or in conjunction with biofeedback. It is important not to start physical therapy or biofeedback until the vestibular Q-tip testing has improved (i.e., the gland scores have decreased). Starting these therapies too soon will likely inhibit results and give woman a sense of failure.
“Since stress plays a role in vulvodynia, any stress-reduction technique, such as meditation and yoga, can be used. Some have found acupuncture helpful. Psychotherapy can be useful because this is a chronic-pain state and women often suffer with depression or relationship problems. It is especially important to let patients know that you understand their problem is a real and debilitating condition, not just “in their heads.”
“The last option for women suffering from localized vulvodynia is vestibulectomy. This should be considered only after all other options have failed.
“It is thought that there can be overlap between vulvodynia and IC. Studies suggest that the prevalence of concurrent IC and vulvodynia ranges from 12% to 68%. Both IC and vulvodynia are syndromes of the urogenital sinus, including pelvic-floor muscle dysfunction, inflammatory changes with activation of mast cells, increased angiogenesis, and neural hyperplasia.”
Reference
Hibner, M., Desai, N., Robertson, L. J., & Nour, M. (2010). Pudendal neuralgia. Journal of minimally invasive gynecology, 17(2), 148-153. Retrieved from https://doi.org/10.1016/j.jmig.2009.11.003
Polycystic Ovarian Syndrome (PCOS)
While two separate issues, there is an association between endometriosis and polycystic ovarian syndrome (PCOS) (Holoch et al., 2014; Hager et al., 2019). There isn’t much data on the incidence of endometriosis and PCOS together. One study noted it to occur in about 19.7% (Holoch et al., 2014).
Below you will find a few links and studies on PCOS.
Links:
Studies:
- Conway, G., Dewailly, D., Diamanti-Kandarakis, E., Escobar-Morreale, H. F., Franks, S., Gambineri, A., … & Pfeifer, M. (2014). The polycystic ovary syndrome: a position statement from the European Society of Endocrinology. European journal of endocrinology, 171(4), P1-P29. Retrieved from https://eje.bioscientifica.com/view/journals/eje/171/4/P1.xml
- Kotsa, K., Yavropoulou, M. P., Anastasiou, O., & Yovos, J. G. (2009). Role of vitamin D treatment in glucose metabolism in polycystic ovary syndrome. Fertility and sterility, 92(3), 1053-1058. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0015028208032809
- Laganà, A. S., Vitale, S. G., Noventa, M., & Vitagliano, A. (2018). Current management of polycystic ovary syndrome: from bench to bedside. International journal of endocrinology, 2018. Retrieved from http://downloads.hindawi.com/journals/ije/2018/7234543.pdf
- Antonio, L., Pauwels, S., Laurent, M. R., Vanschoubroeck, D., Jans, I., Billen, J., … & Vanderschueren, D. (2018). Free testosterone reflects metabolic as well as ovarian disturbances in subfertile oligomenorrheic women. International journal of endocrinology, 2018. Retrieved from https://www.hindawi.com/journals/ije/2018/7956951/
- Díaz, M., Gallego-Escuredo, J. M., López-Bermejo, A., de Zegher, F., Villarroya, F., & Ibáñez, L. (2018). Low-dose spironolactone-pioglitazone-metformin normalizes circulating fetuin-a concentrations in adolescent girls with polycystic ovary syndrome. International Journal of Endocrinology, 2018. Retrieved from https://www.hindawi.com/journals/ije/2018/4192940/
References
Holoch, K. J., Savaris, R. F., Forstein, D. A., Miller, P. B., Higdon III, H. L., Likes, C. E., & Lessey, B. A. (2014). Coexistence of polycystic ovary syndrome and endometriosis in women with infertility. Journal of Endometriosis and Pelvic Pain Disorders, 6(2), 79-83. Retrieved from https://www.researchgate.net/publication/269038400_Coexistence_of_polycystic_ovary_syndrome_and_endometriosis_in_women_with_infertility
Hager, M., Wenzl, R., Riesenhuber, S., Marschalek, J., Kuessel, L., Mayrhofer, D., … & Ott, J. (2019). The prevalence of incidental endometriosis in women undergoing laparoscopic ovarian drilling for clomiphene-resistant polycystic ovary syndrome: a retrospective cohort study and meta-analysis. Journal of clinical medicine, 8(8), 1210. doi: 10.3390/jcm8081210
Fibroids (Leiomyomas)
Fibroids (Leiomyomas) and Endometriosis
Studies:
- Uimari, O., Järvelä, I., & Ryynänen, M. (2011). Do symptomatic endometriosis and uterine fibroids appear together?. Journal of human reproductive sciences, 4(1), 34. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136067/
“Uterine fibroids were detected in 25.8% (47/182) of patients with endometriosis. Endometriosis was detected in 19.6% (47/240) of patients with uterine fibroids. 5.5% (10/183) women undergoing sterilization had endometriosis and 19.3% (17/183) had uterine fibroids. Both uterine fibroids and endometriosis were, independently of each other, related to subfertility (OR, 95% CI: 3.8, 2.3–6.5; 6.8, 4.0–11.6, respectively).”
- Huang, J. Q., Lathi, R. B., Lemyre, M., Rodriguez, H. E., Nezhat, C. H., & Nezhat, C. (2010). Coexistence of endometriosis in women with symptomatic leiomyomas. Fertility and sterility, 94(2), 720-723. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0015028209006207
“Of the 131 patients, 113 were diagnosed with endometriosis and fibroids, while 18 were diagnosed with fibroids alone. Patients with fibroids were on average 4.0 years older than those with endometriosis and fibroids (41 vs. 45). Patients with both diagnoses were also more likely to present with pelvic pain and nulliparity than those with fibroids alone. Conclusion(s): An overwhelming majority of patients with symptomatic fibroids were also diagnosed with endometriosis. Overlooking the concomitant diagnosis of endometriosis in these women may lead to suboptimal treatment of the patients. Further studies are needed to evaluate the impact of surgical treatments on symptom resolution.”
“Aims – Endometriosis is a disease with an unknown pathogenesis that can lead to infertility. Endometrial polyps, fibroids, and polycystic ovarian syndrome (PCOS) have relatively high frequency and are causes of infertility. We hypothesized a possible relationship between the presence of polyps, fibroids, and PCOS in infertile women with endometriosis who underwent laparoscopy and did not get pregnant, compared to women in the control group. Methods – This study was a cross-sectional study of 1,243 infertile patients (621 with endometriosis and 622 controls). Endometriosis, body mass index (BMI), infertility duration, age, and smoking habits were analyzed in relation to the presence of endometrial polyps, fibroids, and PCOS. Results – Polyps, 1.8 (95% CI 1.3 – 2.5); fibroids, 2.5 (95% CI 1.5 – 4.1); and PCOS, 1.0 (95% CI 0.6 – 1.6 were observed in the endometriosis group. A total of 285 patients (45.9%) were classified presenting endometriosis grades I and II, and 336 patients (54.1%) with grades III and IV. Our findings showed a significant association between the presence of fibroids in 129 women with endometriosis (20.8%), and in 69 (53.9%) with endometriosis grades III and IV (p = 0:04). Among the 31 PCOS patients, 24 (77.4%) showed grades I and II (p <0.001). Conclusions – Endometriosis and infertility are associated with the presence of polyps and fibroids. Furthermore, associations between the presence of fibroids with endometriosis grades III and IV, and presence of PCOS with grades I and II were observed.”
Pelvic Floor Dysfunction
“Pelvic pain and abnormal pelvic floor muscle (PFM) tension frequently are present in individuals with endometriosis and often persist even after surgical excision of the endometriosis lesions” (Hunt, 2019).
Links:
- “The Significance of Pelvic Floor Dysfunction”
- “Five things that pelvic health physical therapy can do to improve your endometriosis-related pain”
Studies:
- Aredo, J. V., Heyrana, K. J., Karp, B. I., Shah, J. P., & Stratton, P. (2017, January). Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. In Seminars in reproductive medicine (Vol. 35, No. 01, pp. 088-097). Thieme Medical Publishers. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5585080/
“Given that endometriosis is a disease in which hormonally dependent, inflammatory, ectopic endometrial lesions engage the reproductive, endocrine, vascular, musculoskeletal, and neuronal systems, there are several factors that may contribute to CPP….Since a myofascial source may contribute to endometriosis-associated CPP even after hormonal and surgical treatment has been undertaken, a growing number of practitioners are exploring pain management methods that directly address myofascial pain.”
- Weiss, P. M., Rich, J., & Swisher, E. (2012). Pelvic floor spasm: the missing link in chronic pelvic pain. Contemporary OB/GYN. Retrieved from https://www.contemporaryobgyn.net/view/pelvic-floor-spasm-missing-link-chronic-pelvic-pain
“Acute or chronic pelvic pain is often due to musculoskeletal disorders, which may go unrecognized during a traditional pelvic examination. Proper evaluation facilitates the diagnosis of spasm or trigger points, and physical therapy often achieves a major improvement in quality of life for these women. Pelvic floor musculoskeletal disorders are common in women and too often go unrecognized during the evaluation of pelvic pain syndromes. Although well described in the literature, these disorders cause diverse symptoms that may be missed by a traditional examination of the cervix, uterus, and adnexa. Screening the inferolateral pelvic floor musculature during a routine pelvic examination is very useful for identifying spasm and trigger points contributing to, or resulting from, a patient’s pelvic pain. A brief palpation of the posterior and lateral pelvis to identify spasm in the levator ani (pubococcygeus, iliococcygeus, and puborectalis) often identifies components of pelvic pain that may be dramatically improved by physical therapy and other interventions.”
- Faubion, S. S., Shuster, L. T., & Bharucha, A. E. (2012, February). Recognition and management of nonrelaxing pelvic floor dysfunction. In Mayo Clinic Proceedings (Vol. 87, No. 2, pp. 187-193). Elsevier. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0025619611000243
“Unlike in pelvic floor disorders caused by relaxed muscles (eg, pelvic organ prolapse or urinary incontinence, both of which often are identified readily), women affected by nonrelaxing pelvic floor dysfunction may present with a broad range of nonspecific symptoms. These may include pain and problems with defecation, urination, and sexual function, which require relaxation and coordination of pelvic floor muscles and urinary and anal sphincters. These symptoms may adversely affect quality of life.”
- Orr, N. L., Noga, H., Williams, C., Allaire, C., Bedaiwy, M. A., Lisonkova, S., … & Yong, P. J. (2018). Deep dyspareunia in endometriosis: Role of the bladder and pelvic floor. The journal of sexual medicine, 15(8), 1158-1166. Retrieved from https://dl.uswr.ac.ir/bitstream/Hannan/73785/1/2018%20JSM%20Volume%2015%20Issue%208%20August%20%283%29.pdf
“In women with Stage I/II or Stage III/IV endometriosis, severity of deep dyspareunia was strongly associated with bladder/pelvic floor tenderness and painful bladder syndrome, independent of endometriosis-specific factors, which suggests the role of myofascial or sensitization pain mechanisms in some women with deep dyspareunia.”
- Tu, F. & As-Sanie, S. (2019). Patient education: Chronic pelvic pain in women (Beyond the Basics). Retrieved from https://www.uptodate.com/contents/chronic-pelvic-pain-in-women-beyond-the-basics/print
“Pelvic floor physical therapy (PT) is often helpful for women with abdominal myofascial pain or with pelvic floor pain. This type of PT aims to release the tightness in these muscles by manually “releasing” the tightness; treatment is directed to the muscles in the abdomen, vagina, hips, thighs, and lower back. Physical therapists who perform this type of PT must be specially trained.”
Reference
Hunt, J. B. (2019). Pelvic Physical Therapy for Chronic Pain and Dysfunction Following Laparoscopic Excision of Endometriosis: Case Report. Internet Journal of Allied Health Sciences and Practice, 17(3), 10. Retrieved from https://nsuworks.nova.edu/cgi/viewcontent.cgi?article=1684&context=ijahsp
Interstitial Cystitis/Bladder Pain Syndrome
Not all pelvic pain is endometriosis.
Interstitial Cystitis/Bladder Pain Syndrome – a common cause of pelvic pain in individuals with endometriosis.
Individuals with endometriosis and pelvic pain frequently have more than one condition that contributes to their pelvic pain.
What is Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS)
Definition from the American Urological Association UC/PBS Treatment Guideline:
“An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than six weeks duration, in the absence of infection or other identifiable causes.” (https://www.auanet.org/guidelines/interstitial-cystitis/bladder-pain-syndrome-(2011-amended-2014)#4)
The AUA selected this definition because it allows treatment to begin after a relatively short symptomatic period, preventing treatment delays that could occur with definitions that require longer symptom durations (i.e., six months). The AUA recommends clinicians (as opposed to researchers) against using strict definitions used in research or clinical trials because many patients may experience misdiagnosis or delays in diagnosis resulting in delays in treatment.
Symptoms
From RAND IC Epidemiology (RICE) Study:
“Pain, pressure or discomfort in the pelvic area AND daytime urinary frequency of 10+ OR urgency due to pain, pressure, or discomfort, not fear of wetting.”
Treatment
There is not a “one size fits most” treatment for IC/BPS. There are many treatment options and most individuals require more than one treatment at the same time to relieve symptoms. For example, an individual may need to avoid dietary triggers, have physical therapy, and take over counter medications. Another individual may need to avoid dietary triggers and have medications instilled in their bladder periodically. Finding the right combination of treatments requires that individuals with IC/BPS engage with their health care team and exercise patience as they and their team work through various treatment combinations. A great first step is to educate oneself about IC/BPS.
Links:
- Overview of IC/BPS from the Urology Care Foundation: Interstitial cystitis/bladder pain syndrome (IC/BPS)
- Overview of treatment from Interstitial Cystitis Association: https://www.ichelp.org/wp-content/uploads/2015/05/AUA-IC-Guideline-September-2014-Update-final.pdf
- Full guidelines from the America Urological Association: https://www.auanet.org/common/pdf/education/clinical-guidance/IC-Bladder-Pain-Syndrome-Revised.pdf
Symptom questionnaire:
Pelvic Pain and Urgency/Frequency (PUF)Patient Symptom scale: This tool assists clinicians in diagnosing IC/BPS and monitoring response to interventions. Remember that this is just one piece of information in a detailed evaluation.
Diet:
Patients with IC/BPS often have dietary triggers and can vary among patients. It is important to explore and identify your dietary triggers. Consider keeping a detailed journal to help identify dietary triggers.
Commonly reported triggers:
- Coffee, tea, soda, alcohol, citrus juices, and cranberry juice
- Foods and beverages containing artificial sweeteners
- Hot peppers and spicy foods
- Many nuts
- Carbonated beverages
- Tomatoes
- Soy
- MSG (monosodium glutamate)***
***Monosodium glutamate is frequently contained in foods and not always labeled because there are over 40 ingredients in foods can contain MSG/Free glutamic acid. MSG is highly prevalent in processed foods, even organic processed foods and restaurant foods.
Links on Nutrition:
- Hidden sources of MSG: http://www.truthinlabeling.org/hiddensources.html
- Dietary trigger avoidance from the Interstitial Cystitis Association: https://www.ichelp.org/living-with-ic/interstitial-cystitis-and-diet/foods-to-avoid/
- IC and food sensitivities by Erin Luyendyk, RHN: http://www.thenutritionista.ca/ic-and-food-sensitivities/
- Nutrition overview by Erin Luyendyk, RHN: ENDOMETRIOSIS & NUTRITION
Additional Resources
- American Urological Association guidelines for IC/BPS: https://www.auanet.org/guidelines/interstitial-cystitis-(ic/bps)-guideline
- Interstitial Cystitis Association: https://www.ichelp.org
- Urology Care Foundation: https://www.urologyhealth.org/urologic-conditions/interstitial-cystitis
- Overview of IC/BPS from an endometriosis expert: http://pacificendometriosis.com/interstitial-cystitis/
Endometrial/Uterine Polyps
An endometrial or uterine polyp is an abnormal growth on the inner wall of the uterus. They either arise from the uterine wall by a stem (think of a tree) or directly, and they can be as small as a seed or fill the entire uterine cavity. They have been reported to be sensitive to the effects of estrogen (Nijkang, Anderson, Markham, & Manconi, 2019). They may be asymptomatic, but they can cause irregular bleeding (like spotting in between periods or bleeding in post-menopausal women), heavier bleeding, and/or cramp-like pain. Endometriosis patients are much more likely to have endometrial polyps (Shen et al., 2011).
Endometriosis and endometrial/uterine polyps:
- Shen, L., Wang, Q., Huang, W., Wang, Q., Yuan, Q., Huang, Y., & Lei, H. (2011). High prevalence of endometrial polyps in endometriosis-associated infertility. Fertility and sterility, 95(8), 2722-2724. Retrieved from https://pubmed.ncbi.nlm.nih.gov/21575952/
“In a retrospective study, examination of 431 infertile women (158 cases with endometriosis and 273 without endometriosis) showed a significantly increased frequency of endometrial polyps in patients with endometriotic infertility and no significant differences among different stages and locations of endometriosis.”
- Kim, M. R., Kim, Y. A., Jo, M. Y., Hwang, K. J., & Ryu, H. S. (2003). High frequency of endometrial polyps in endometriosis. The Journal of the American Association of Gynecologic Laparoscopists, 10(1), 46-48. Retrieved from https://www.jmig.org/article/S1074-3804(05)60233-2/abstract
“We strongly recommend hysteroscopy if endometriosis is detected in a woman undergoing evaluation for infertility, even if hysterosalpingography and transvaginal ultrasonography do not suggest endometrial polyps.”
- Park, J. S., Lee, J. H., Kim, M., Chang, H. J., Hwang, K. J., & Chang, K. H. (2009). Endometrium from women with endometriosis shows increased proliferation activity. Fertility and sterility, 92(4), 1246-1249. Retrieved from https://www.fertstert.org/article/S0015-0282(09)00869-3/pdf
“Examination of 631 infertile women, including 434 women with endometriosis and 197 without endometriosis, revealed an increasing incidence of endometrial polyps, especially in the test subjects with endometriosis, and advanced stages of endometriosis. Expression of Ki-67 and Bcl-2 proteins and MTT assay results were significantly higher in endometrium of patients with endometriosis than in patients without endometriosis. These showed increased proliferation activity and cell proliferation markers not only clinically but also pathologically.”
- Indraccolo, U., & Barbieri, F. (2011). Relationship between adenomyosis and uterine polyps. European Journal of Obstetrics & Gynecology and Reproductive Biology, 157(2), 185-189. Retrieved from https://pubmed.ncbi.nlm.nih.gov/21470766/
“The presence of multiple endometrial polyps seemed to be associated with the presence of adenomyosis (p=0.016). The presence of cervical polyps was significantly associated only with presence of adenomyosis (p=0.002). The results clearly demonstrate an association between adenomyosis and uterine polyps. The pathogenetic role of adenomyosis in the development of polyps should therefore be investigated further.”
References
Nijkang, N. P., Anderson, L., Markham, R., & Manconi, F. (2019). Endometrial polyps: pathogenesis, sequelae and treatment. SAGE open medicine, 7, 2050312119848247. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6501471/
Shen, L., Wang, Q., Huang, W., Wang, Q., Yuan, Q., Huang, Y., & Lei, H. (2011). High prevalence of endometrial polyps in endometriosis-associated infertility. Fertility and sterility, 95(8), 2722-2724. Retrieved from https://pubmed.ncbi.nlm.nih.gov/21575952/
Adenomyosis
What is Adenomyosis?
Adenomyosis can be another cause of chronic pelvic pain. Adenomyosis is a condition where tissue like the lining of the uterus invades the muscle of the uterus. It can be either diffuse or focal, meaning it can spread out over the uterus or can be grouped together (Agostinho et al., 2017). According to Chapron et al. (2020), the symptoms of adenomyosis can include:
- heavy menstrual bleeding
- painful periods and menstrual cramps (medical term: dysmenorrhea)
- abnormal uterine bleeding
- bloating
- pain with sex (before, during, and/or after) (medical term: dyspareunia)
- pelvic pain
- infertility
- miscarriage
Many of these symptoms overlap with endometriosis. Endometriosis and adenomyosis share similar characteristics of sex steroid hormones abnormalities, inflammation, neurogenesis (growth of new nerves), and angiogenesis (growth of new blood vessels) (Gordts, Grimbizis, & Campo, 2018). However, there are differences between the two that leave researchers concluding that adenomyosis is its own separate disease process from endometriosis (Vannuccini et al., 2017).
Adenomyosis might be suspected and a transvaginal ultrasound (TVUS) or magnetic resonance imagining (MRI) performed. Some studies have suggested that MRI might be more accurate in detecting adenomyosis (Bazot & Daraï, 2018). A biopsy is the definitive way to diagnosis adenomyosis- its accuracy improved by the use of an ultrasound guided biopsy (Nam & Lyu, 2015).
“The standard treatment of adenomyosis is hysterectomy, but there is no medical therapy to treat the symptoms of adenomyosis while still allowing patients to conceive. Medical therapies using suppressive hormonal treatments, such as continuous use of oral contraceptive pills, high-dose progestins, selective oestrogen receptor modulators, selective progesterone receptor modulators, the levonorgestrel-releasing intrauterine device, aromatase inhibitors, danazol, and gonadotrophin receptor hormone agonists can temporarily induce regression of adenomyosis and improve the symptoms.” (Pontis et al., 2016)
There are also surgical options which do not involve a hysterectomy, such as “(1) complete excision of adenomyosis, (2) cytoreductive surgery or incomplete removal of the lesion, or (3) nonexcisional techniques” (Grimbizis, Mikos, & Tarlatzis, 2014).
References
- Agostinho, L., Cruz, R., Osório, F., Alves, J., Setúbal, A., & Guerra, A. (2017). MRI for adenomyosis: a pictorial review. Insights into imaging, 8(6), 549-556. Retrieved from https://insightsimaging.springeropen.com/articles/10.1007/s13244-017-0576-z
- Bazot, M., & Daraï, E. (2018). Role of transvaginal sonography and magnetic resonance imaging in the diagnosis of uterine adenomyosis. Fertility and sterility, 109(3), 389-397. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0015028218300244
- Chapron, C., Vannuccini, S., Santulli, P., Abrão, M. S., Carmona, F., Fraser, I. S., … & Pistofidis, G. (2020). Diagnosing adenomyosis: an integrated clinical and imaging approach. Human Reproduction Update, 26(3), 392-411. Retrieved from https://academic.oup.com/humupd/article-abstract/26/3/392/5756142
- Gordts, S., Grimbizis, G., & Campo, R. (2018). Symptoms and classification of uterine adenomyosis, including the place of hysteroscopy in diagnosis. Fertility and sterility, 109(3), 380-388. Retrieved from https://link.springer.com/article/10.1007/s40271-017-0284-2
- Grimbizis, G. F., Mikos, T., & Tarlatzis, B. (2014). Uterus-sparing operative treatment for adenomyosis. Fertility and sterility, 101(2), 472-487. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0015028213031713
- Nam, J. H., & Lyu, G. S. (2015). Abdominal ultrasound-guided transvaginal myometrial core needle biopsy for the definitive diagnosis of suspected adenomyosis in 1032 patients: a retrospective study. Journal of minimally invasive gynecology, 22(3), 395-402. Retrieved from https://www.sciencedirect.com/science/article/pii/S1553465014004129
- Pontis, A., D’alterio, M. N., Pirarba, S., De Angelis, C., Tinelli, R., & Angioni, S. (2016). Adenomyosis: a systematic review of medical treatment. Gynecological Endocrinology, 32(9), 696-700. Retrieved from https://www.tandfonline.com/doi/abs/10.1080/09513590.2016.1197200
- Vannuccini, S., Tosti, C., Carmona, F., Huang, S. J., Chapron, C., Guo, S. W., & Petraglia, F. (2017). Pathogenesis of adenomyosis: an update on molecular mechanisms. Reproductive biomedicine online, 35(5), 592-601. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S1472648317302961
Links:
- Adenomyosis Support Group: https://www.facebook.com/groups/AdenomyosisSupport/
- “Adenomyosis – Sister To Endometriosis Or Distant Cousin?”
- “Adenomyosis”
- “Endometriosis and Adenomyosis: Decoding Their Contribution To Pelvic Pain”
- “Adenomyosis: is it really endometriosis?”
- “Presacral Neurectomy”
- “What are the indications for hysterectomy?”
Studies:
- Jiang, C., & Cheng, Z. (2016). Update of recent studies of adenomyosis-associated dysmenorrhea. Gynecology and Minimally Invasive Therapy, 5(4), 137-140. Retrieved from https://www.sciencedirect.com/science/article/pii/S2213307016300387
- Donnez, J., Dolmans, M. M., & Fellah, L. (2019). What if deep endometriotic nodules and uterine adenomyosis were actually two forms of the same disease?. Fertility and sterility, 111(3), 454-456. Retrieved from https://www.fertstert.org/article/S0015-0282(18)32307-0/abstract
- Onchee, Y. U., Schulze-Rath, R., Grafton, M. J., Hansen, M. K., & Scholes, D. (2020). Adenomyosis incidence, prevalence and treatment: united states population-based study 2006-2015. American Journal of Obstetrics and Gynecology. Retrieved from https://www.ajog.org/article/S0002-9378(20)30023-5/fulltext?fbclid=IwAR0vRX3OQnfmq0v9f6jFw-jHbVOq8uuu0n8LKdS1eTOEofrhqmZWPle1PFw

Adenomyosis and Endometriosis, Differences and Similarities
Adenomyosis and endometriosis, two different yet similar conditions, have long challenged the medical community with their manifestations and elusive origins. While sharing some similarities, these disorders have characteristics that demand meticulous examination and unique approaches to management. This article discusses adenomyosis and endometriosis, their differences, symptoms, causes, and cutting-edge diagnostic and therapeutic avenues.
Table of contents
- Understanding the Fundamental Differences Between Endometriosis and Adenomyosis
- The Spectrum of Symptoms
- The Disease’s Origins and Potential Causes
- Diagnosing Endometriosis vs. Adenomyosis
- Treatments
- Fertility Implications
- Coping Mechanisms
- Research and Cutting-Edge Advancements
- Raising Awareness
- A Multidisciplinary Approach: Collaborating for Comprehensive Care
- A Journey That Needs Hope and Resilience
Understanding the Fundamental Differences Between Endometriosis and Adenomyosis
A crucial distinction lies at the heart of these conditions: the location of the disease growth. In adenomyosis, the endometrial cells, which typically line the uterine cavity, infiltrate and embed themselves within the muscular walls of the uterus itself. This invasion results in a thickening of the uterine walls, causing potential complications.
Conversely, endometriosis involves the abnormal proliferation of endometrial-like tissue beyond the uterus, often colonizing surrounding organs such as the ovaries, fallopian tubes, and even the bladder or intestines. This misplaced tissue behaves similarly to the endometrium, undergoing cyclic shedding and bleeding, which can lead to the formation of adhesions, cysts, and scarring within the affected areas.
The Spectrum of Symptoms
While adenomyosis and endometriosis share some common symptoms, there are distinct nuances that can help in their differentiation. Both conditions can manifest as pelvic pain, particularly during menstrual cycles, as well as heavy or irregular bleeding patterns. However, adenomyosis may present with an enlarged, tender uterus, while endometriosis can cause pain during bowel movements, urination, or sexual intercourse, depending on the location of the endometrial implants.
The Disease’s Origins and Potential Causes
Despite extensive research, the exact causes of adenomyosis and endometriosis remain unclear. However, certain risk factors have been identified that may increase an individual’s susceptibility to these conditions.
For adenomyosis, factors such as prior uterine surgeries, multiple pregnancies, and increased exposure to estrogen have been implicated as potential contributors. Endometriosis, on the other hand, has been linked to a family history of the condition, early onset of menstruation (before age 11), short menstrual cycles (less than 27 days), and heavy periods lasting more than seven days.
Two widely discussed reasons for the development of endometriosis are cell misplacement during organogenesis and retrograde menstruation. However, the exact mechanisms underlying the development of both conditions remain elusive, highlighting the need for further research.
Diagnosing Endometriosis vs. Adenomyosis
Diagnosing adenomyosis and endometriosis can be a complex and multifaceted process, often requiring a combination of various diagnostic tools and techniques.
For adenomyosis, imaging modalities such as transvaginal ultrasound and magnetic resonance imaging (MRI) can provide valuable insights into the thickness and texture of the uterine walls, potentially revealing the presence of abnormal growths or cysts. However, in some cases, a definitive diagnosis may only be possible by examining uterine tissue samples obtained during a hysterectomy or biopsy.
Endometriosis, on the other hand, frequently requires a surgical procedure known as laparoscopy. During this minimally invasive procedure, a tiny camera is inserted into the abdominal cavity, enabling the surgeon to inspect for the presence of endometriosis implants visually and, if necessary, obtain tissue samples for further analysis.
While imaging techniques like ultrasound and MRI can suggest the presence of endometriosis, they may not always detect smaller lesions or implants, making laparoscopy the gold standard for definitive diagnosis.
Treatments
The management of adenomyosis and endometriosis is a highly individualized process tailored to each patient’s unique circumstances, symptom severity, and fertility goals. For both conditions, initial treatment often involves over-the-counter pain medications, such as nonsteroidal anti-inflammatory drugs (NSAIDs), to alleviate discomfort and manage heavy bleeding. Hormonal contraceptives, including birth control pills, progestin-only intrauterine devices (IUDs), and gonadotropin-releasing hormone (GnRH) agonists, can also be employed to regulate menstrual cycles and suppress the growth of endometrial tissue.
In cases where medical management proves inadequate, surgical interventions may be considered. For adenomyosis, options include robotic-assisted excision of the affected uterine tissue or, in severe cases, a hysterectomy (removal of the uterus). Endometriosis similarly requires laparoscopic surgery to remove endometriosis implants and adhesions or, in some instances, a hysterectomy with bilateral salpingo-oophorectomy (removal of the uterus, fallopian tubes, and ovaries).
It is crucial to note that while surgery can alleviate symptoms, it does not necessarily cure endometriosis, as the condition may recur. Ongoing management and close monitoring are often necessary to ensure optimal outcomes.
Fertility Implications
Both adenomyosis and endometriosis can have profound impacts on an individual’s fertility and reproductive health. Endometriosis, in particular, is a leading cause of infertility and subfertility, as the presence of endometriosis implants and adhesions can impede ovulation, disrupt the fallopian tube function, and create an inhospitable environment for embryo implantation. In cases of adenomyosis, the abnormal thickening of the uterine walls can make it challenging for embryos to implant successfully, increasing the risk of miscarriage or complications during pregnancy.
A multidisciplinary approach involving fertility specialists and gynecologists may be necessary for individuals seeking to conceive. Treatment options may include assisted reproductive technologies (ART) such as in vitro fertilization (IVF), intrauterine insemination (IUI), or the use of fertility medications to induce ovulation. In severe cases of adenomyosis or endometriosis, where fertility preservation is not a priority, a hysterectomy or other surgical interventions may be recommended to alleviate symptoms and improve overall quality of life.
Coping Mechanisms
Living with chronic conditions like adenomyosis and endometriosis can be emotionally and physically taxing, often leading to feelings of anxiety, depression, and a diminished sense of well-being. A holistic approach that addresses these conditions’ physical and psychological aspects can be instrumental in improving overall quality of life.
In addition to medical interventions, complementary therapies such as routine exercise, meditation, massage, and acupuncture can be beneficial for managing pain and reducing stress levels associated with adenomyosis and endometriosis.
Furthermore, seeking support from professional counselors, therapists, or support groups can provide a valuable outlet for individuals to share their experiences, receive emotional support, and learn coping strategies from others navigating similar journeys.
Research and Cutting-Edge Advancements
The field of gynecological research is constantly evolving, with scientists and clinicians tirelessly exploring innovative approaches to understanding, diagnosing, and treating adenomyosis and endometriosis.
One promising avenue is the development of non-invasive diagnostic techniques, such as advanced imaging modalities or biomarker analysis, which could eliminate the need for invasive procedures like laparoscopy in some cases.
Additionally, ongoing research into these conditions’ genetic and molecular underpinnings may yield insights into novel therapeutic targets and personalized treatment strategies tailored to an individual’s unique genetic profile.
Furthermore, advancements in robotic-assisted surgical techniques and minimally invasive procedures continue to enhance precision, reduce recovery times, and minimize the risk of complications associated with traditional surgical interventions.
Raising Awareness
Despite their prevalence, adenomyosis and endometriosis often remain misunderstood and overlooked, leading to delays in diagnosis and inadequate support for patients.
Raising awareness about these conditions is crucial in empowering patients to advocate for their health, seek timely medical attention, and spread understanding within their personal and professional circles.
Everyone should consider promoting open dialogue, sharing personal experiences, and collaborating with healthcare professionals, advocates, and support organizations. By doing so, we can break down barriers, challenge misconceptions, and ensure that individuals affected by adenomyosis and endometriosis receive the compassionate care and support they deserve.
A Multidisciplinary Approach: Collaborating for Comprehensive Care
Endometriosis and adenomyosis are complex. Therefore, they demand a comprehensive and multidisciplinary approach involving various specialties.
Gynecologists, physical therapists, pain management specialists, mental health professionals, and fertility experts are the pieces that can help. These experts must collaborate to develop individualized treatment plans that address each patient’s unique needs and goals.
This multidisciplinary team can provide holistic care through open communication and a collaborative mindset. Holistic care can cover medical management, psychological support, and fertility preservation strategies. The multidisciplinary team and holistic care ensure the best possible outcomes for patients.
A Journey That Needs Hope and Resilience
The challenges posed by adenomyosis and endometriosis can be daunting. Therefore, it is essential to have hope and resilience throughout the journey. These conditions, though chronic, are manageable. Individuals can reclaim control over their lives and pursue their dreams with the proper support, management strategies, and a positive mindset.
In conclusion, the complex nature of adenomyosis and endometriosis demands a multifaceted approach that combines science, compassion, and a deep understanding. By collaboration, raising awareness, and innovative solutions, we can overcome this disease now and in the future.
Endometriosis and Adhesions: Correlations and Treatments
Table of contents
What is Endometriosis?
Endometriosis is a complex disorder characterized by the growth of endometrial-like tissue (the tissue that usually lines the uterus) in locations outside the uterine cavity. This misplaced tissue behaves similarly to the endometrium, thickening, breaking down, and bleeding with each menstrual cycle. However, unlike the endometrium, which is expelled during menstruation, the displaced endometrial tissue cannot exit the body, leading to inflammation, scarring, and the formation of adhesions.
Understanding Adhesions
Adhesions are fibrous bands of scar tissue that form abnormal connections between typically separate organs or tissues. Although they can form anywhere in the body, they are most frequently found in the pelvic area when endometriosis is present, binding organs like the uterus, fallopian tubes, ovaries, and intestines.
Causes of Adhesions in Endometriosis
One major contributing factor to the formation of adhesions in the pelvic cavity is endometriosis. Adhesions may occur as a result of the inflammatory process that endometriotic lesions cause via the following mechanisms:
- Bleeding and Inflammation: Endometriotic lesions have the potential to bleed during menstruation, which can trigger an inflammatory reaction in the tissues around them. Scar tissue that forms due to this inflammation may stick to adjacent organs or tissues.
- Surgical Interventions: Endometriosis patients frequently require surgery to manage related problems or remove endometriotic lesions. Certain surgical treatments can unintentionally cause adhesions to form while the body repairs itself.
- Endometriotic Implants: There is a chance that endometriotic implants will encourage the formation of adhesions. As the implants grow and mature, they may adhere to the surrounding tissues, creating fibrous bands that keep organs together.
Differentiating Between Adhesion Pain and Endometriosis Pain
Adhesions and endometriosis are comparable conditions that frequently coexist. However, there may be some distinctions. The inflammatory process that takes place inside the endometriotic lesions itself is directly related to endometriosis discomfort. Adhesion discomfort, on the other hand, results from the binding and restricted movement of organs because of the scar tissue’s fibrous bands.
Effect on Life Quality
Endometriosis and adhesions both severely impair a woman’s quality of life and are frequently linked to infertility, chronic pelvic discomfort, and other issues. Adhesions can cause organ displacement, intestinal blockages, and disturbances to normal physiological functioning, all of which can worsen the symptoms of endometriosis. They may also make endometriosis surgeries more difficult since they may mask endometriotic lesions and complicate surgical procedures.
Diagnosis and Treatment
Diagnosing Endometriosis Adhesions
It can be difficult to diagnose adhesions linked to endometriosis. Although laparoscopic or open surgery is frequently necessary for a conclusive diagnosis, adhesions may be better understood by using imaging methods like magnetic resonance imaging (MRI) and ultrasound.
The surgeon can visually evaluate the pelvic cavity during a laparoscopic operation to check for adhesions. Adhesions can manifest as thin, filmy, transparent bands or as thick, dense, opaque structures, depending on the severity of the condition.
Treatment Approaches
Adhesions in endometriosis are usually treated with a mix of surgical and pharmaceutical procedures:
- If adhesions are severe and substantially reduce a patient’s quality of life, surgery may be necessary to remove them. This can be accomplished via laparoscopic surgery, depending on the degree and location of the adhesions. Carefully separating the adhesions from the afflicted organs during the surgical operation minimizes stress and stops new adhesion formation. Because they lower the chance of new adhesion creation than open treatments, minimally invasive techniques like laparoscopic surgery are frequently chosen.
- Treatment for Endometriosis: To stop adhesions from recurring, the underlying endometriosis must be addressed. Hormonal therapy is one option for treating endometriosis; it suppresses hormones, reduces inflammation, and treats symptoms. To eliminate the cause of inflammation and lower the chance of adhesion formation, it may occasionally be advised to remove or ablate endometriotic lesions.
It is crucial to remember that the course of therapy should be customized to the needs of each patient, taking into account the degree of adhesions, the severity of endometriosis, and any possible effects on quality of life and fertility.
Endometriosis and Adhesions: A Complex Interaction
Although endometriosis and adhesions are distinct conditions, they frequently coexist and have complex interactions. While endometriosis can result in tissue damage and inflammation that can contribute to the formation of adhesions, adhesions can exacerbate the symptoms of endometriosis and complicate surgical operations.
To manage the associated discomfort, preserve fertility, and improve overall quality of life, women with endometriosis and adhesions require a correct diagnosis and treatment plan. Medical experts can develop comprehensive therapeutic methods tailored to the patient’s needs by understanding these two conditions’ relationships.
Conclusion:
Two distinct illnesses that can have a major effect on a person’s health and quality of life are adhesion and endometriosis. In cases of endometriosis, endometrial-like tissue proliferates extraordinarily, resulting in fibrous scar tissue that may unintentionally stick to other organs. Prolonged pelvic pain; organ displacement; and surgical complications can arise from adhesion formation caused by endometriosis-induced inflammation. For many disorders, selecting the best therapy requires a precise diagnosis and an effective treatment plan that may involve medication and surgery. Knowing the connection between adhesions and endometriosis enables medical professionals to treat patients with greater specialization and comprehensive care, improving their overall health and well-being.
Does Gastrointestinal Endometriosis Cause Infertility
Table of contents
Gastrointestinal endometriosis is a condition that poses numerous health challenges to women, and one of the most concerning questions revolves around its potential impact on fertility. The primary focus of this article is to address the question:
Does gastrointestinal endometriosis cause infertility?
We will dissect this issue by exploring the available medical and scientific evidence.
Understanding Endometriosis and its Symptoms
Endometriosis can manifest with various symptoms, although not all women may experience them. Some common symptoms include:
- Painful periods: Women with endometriosis often experience more intense pelvic pain and cramping before and during their menstrual cycle.
- Chronic lower back/abdominal pain: Another hallmark of endometriosis is persistent pain in the lower back or abdomen.
- Infertility: Endometriosis has been associated with fertility problems, making it more challenging for some women to conceive.
- Excessive bleeding and spotting: Women with endometriosis may experience heavy bleeding during their periods or irregular bleeding between periods due to the presence of adenomyosis.
- Pain during or after intercourse: Endometrial tissue growths can cause pain during sexual intercourse, which can have a significant impact on a woman’s quality of life.
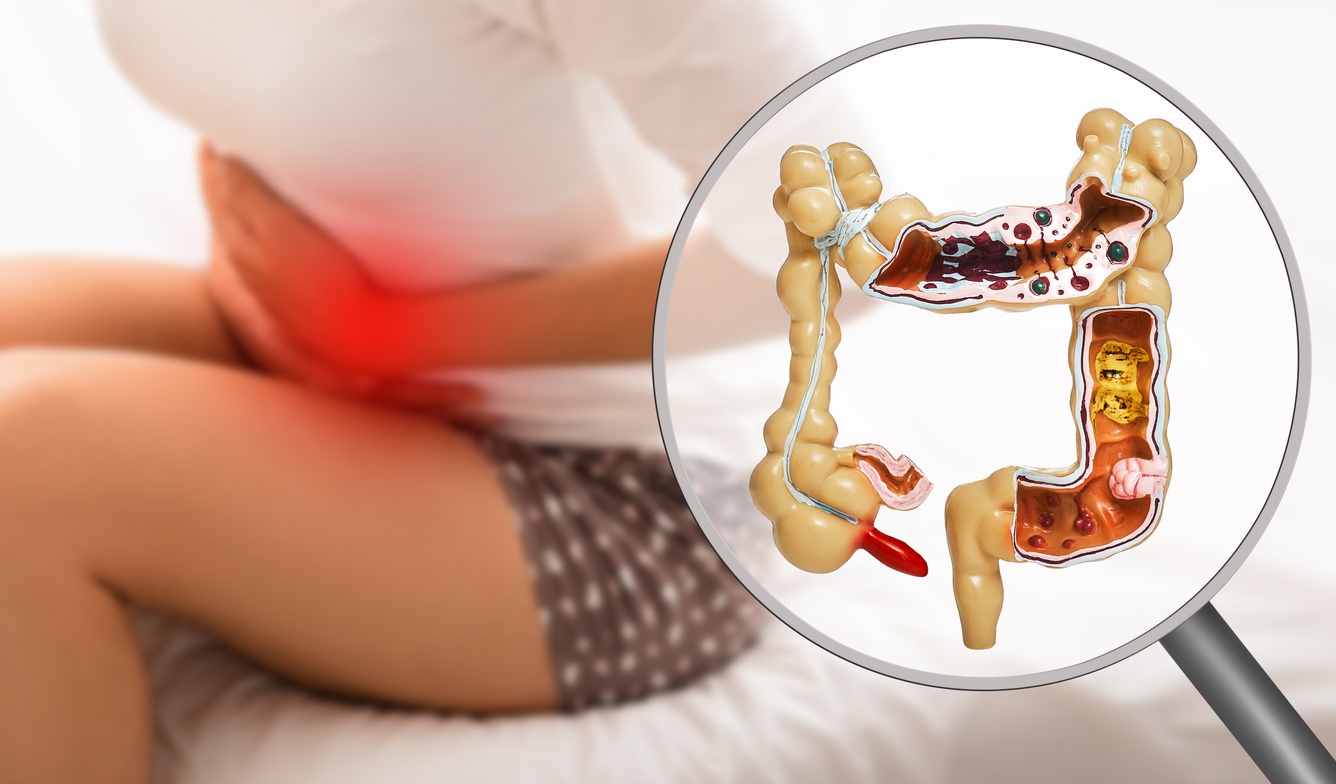
- Gastrointestinal issues: Endometriosis affecting the intestines can lead to symptoms such as painful bowel movements, diarrhea, constipation, and stomach issues like nausea.
- Fatigue: Chronic fatigue is a common complaint among women with endometriosis, which can be attributed to the physical and emotional toll of dealing with the condition.
Endometriosis and Fertility
The relationship between endometriosis and fertility has been a subject of continuous research. Women with endometriosis, particularly moderate to severe forms, often face fertility challenges. However, it’s important to note that endometriosis does not automatically lead to infertility. Many women with endometriosis can and do conceive naturally or with the help of fertility treatments.
How Endometriosis Impacts Fertility
The mechanism through which endometriosis affects fertility is complex and multifaceted. Here are some ways it can potentially interfere with conception:
- Anatomical Distortions: Endometriosis can cause adhesions or scar tissue formation, leading to a distortion of pelvic anatomy. This can block the fallopian tubes or alter the position of the ovaries, hindering the meeting of sperm and egg.
- Inflammatory Environment: Endometriosis creates an inflammatory environment in the pelvic region, which might harm the quality of eggs or sperm and hinder their movement.
- Impact on the Endometrium: Some studies suggest that endometriosis may affect the lining of the uterus (the endometrium), making it less receptive to an implanting embryo.
Gastrointestinal Endometriosis and Infertility: Is there a Connection?
When it comes to the specific question – does gastrointestinal endometriosis cause infertility – the answer is not as straightforward as one might hope. While endometriosis is known to affect fertility in general, the impact of gastrointestinal endometriosis on fertility is less clear.
Evidence suggests that endometriosis involving the bowel or bladder can be more challenging to treat and may require more complex surgical procedures, which could potentially affect reproductive function. However, it’s also important to remember that the presence of gastrointestinal endometriosis does not necessarily mean that a woman will experience fertility problems. However, the inflammation and molecular impacts of endometriosis might still increase the risk of fertility problems.
Treating Gastrointestinal Endometriosis
Medical Treatment
The first line of treatment for endometriosis often involves hormone therapy, such as birth control pills or progestin-based contraceptives, which work by managing symptoms and manipulating hormones. However, these medications do not improve fertility.
Surgical Treatment
Surgery to remove endometriosis patches can potentially improve fertility, especially in cases of moderate to severe endometriosis. However, surgical treatment of gastrointestinal endometriosis can be complex and may carry a higher risk of complications. Depending on the extent of the disease, it may involve resection of a portion of the bowel or bladder.
The Path to Pregnancy with Endometriosis
Surgical treatment can increase the chance of natural and assisted fertility. However, in many cases the patient still needs further support and treatment.
Fertility Treatments
For women with endometriosis who are struggling to conceive, assisted reproductive technologies (ART) such as in-vitro fertilization (IVF) may be an option. While women with severe endometriosis may have a lower success rate with IVF than other women, many are still able to achieve a successful pregnancy with this treatment.
Surrogate pregnancy
There are some options to seek help from other women’s bodies and eggs if necessary and desired.
Maintaining Hope
The journey of dealing with endometriosis and its potential impact on fertility can be emotionally challenging. However, it’s important to maintain hope. Many women with endometriosis, including gastrointestinal endometriosis, are able to conceive and have healthy pregnancies, whether naturally or with the help of fertility treatments.
Final Thoughts
In conclusion, while gastrointestinal endometriosis can pose challenges, it can impact fertility by inflammation and molecular pathways. Each case of endometriosis is unique, and the impact on fertility can vary greatly from one individual to another. If you’re dealing with endometriosis and are concerned about your fertility, it’s important to seek guidance from a healthcare provider who can provide individualized advice based on your specific situation.
Remember, understanding your condition and exploring your options can empower you to make the best decisions for your health and fertility journey. So, while gastrointestinal endometriosis can pose hurdles, they are not insurmountable. With the right treatment and support, the dream of parenthood can still be a reality for many women living with endometriosis.
References:
https://pubmed.ncbi.nlm.nih.gov/32631683/
https://www.obgyn-care.net/blog/does-endometriosis-cause-infertility
