

Colon Chronicles: Delving into Bowel Endometriosis
In our recent blog, we highlighted the significance of addressing bowel endometriosis, a condition prone to misdiagnosis. Whether individuals have struggled with lifelong bowel issues or are suddenly facing disruptions, determining what’s considered normal can be perplexing. The “normal” range spans anywhere from three times a day to as infrequent as three times per week. In many sources, the focus is typically limited to frequency and to some degree consistency; however, there’s an overall scarcity of information on what defines normalcy.
Table of contents
ICYMI: Understanding Bowel Endometriosis
This ambiguity is particularly challenging for those with endometriosis, where gastrointestinal symptoms vary widely, making it tough to discern what’s amiss. About 90% of endometriosis cases involve some form of gastrointestinal symptoms, often leading to an IBS (irritable bowel syndrome) diagnosis, which essentially offers a label for persistent symptoms without an identifiable cause. The usual next step in diagnostics is often a colonoscopy, a key tool for identifying or ruling out certain diseases. This article explores the nuances of bowel endometriosis, with a primary focus on the role and precision of colonoscopy in diagnosing this condition.
Bowel endometriosis is considered to be deep infiltrating endometriosis and can lead to a variety of symptoms which we discussed in the previous blog, but is often concerning if not diagnosed timely and may risk more complex surgeries including resection if the disease is not properly addressed.
Related Reading: How to Get an Endometriosis Diagnosis
The Role of Colonoscopy – Is it helpful?
A colonoscopy is a diagnostic procedure commonly used to examine the inner lining of the large intestine (colon and rectum). It involves the use of a long, flexible tube called a colonoscope, which has a small camera attached to its end. This tool allows physicians to visualize the interior of the colon to identify any abnormal conditions or changes.
In the context of bowel endometriosis, a colonoscopy can potentially detect signs of endometrial tissue growth within the bowel. However, its effectiveness and accuracy in diagnosing this condition have been subjects of ongoing research and debate. Aside from its ability to detect endometriosis, there is also consideration of the provider performing the procedure and their level of knowledge of endometriosis.
The use of colonoscopy in diagnosing bowel endometriosis has been a topic of considerable discussion among medical professionals. Given the invasive nature of the procedure and the often non-specific symptoms of bowel endometriosis, the role and necessity of colonoscopy in its diagnostic process have been questioned.
However, several case studies and research findings suggest that colonoscopy can indeed play a crucial role in identifying bowel endometriosis. In particular, it has been found to be effective in detecting endometriosis growth in the bowel, with certain colonoscopic findings such as eccentric wall thickening, polypoid lesions, and surface nodularities often being associated with endometriosis.
Evaluating the Accuracy of Colonoscopy for Diagnosing Bowel Endometriosis
While the potential of colonoscopy in detecting bowel endometriosis has been recognized, its accuracy in doing so has been the subject of extensive research. A number of studies have sought to evaluate the sensitivity, specificity, and predictive values of colonoscopy in diagnosing this condition.
One such study was conducted by Milone M et al., who performed a prospective observational study that included women diagnosed with deep pelvic endometriosis. The study aimed to evaluate the accuracy of colonoscopy in predicting intestinal involvement in deep pelvic endometriosis.
The results of the study suggested that colonoscopy did have the potential to detect bowel endometriosis, with a number of cases accurately diagnosed through the procedure. However, the overall sensitivity, specificity, and predictive values of colonoscopy were found to be variable, indicating room for improvement in its diagnostic accuracy.
In another study conducted by Marco Milone and his team, the researchers also found that while colonoscopy could indeed identify bowel endometriosis, its accuracy was not optimal. The study elucidated that the presence of colonoscopic findings of intestinal endometriosis in deep pelvic endometriosis was quite low, indicating that routine colonoscopy may not be justified for all women with deep pelvic endometriosis.
A Case Study: Bowel Endometriosis and Colonoscopy
To illustrate the potential role of colonoscopy in diagnosing bowel endometriosis, let’s consider a case study involving a 45-year-old woman who presented with abdominal pain in her left lower quadrant. This woman underwent a colonoscopy, which revealed a submucosal tumor-like lesion in her sigmoid colon.
Upon further examination using magnifying endoscopy, the lesion was found to contain sparsely distributed round pits – a finding that was suggestive of endometrial glands and stroma (the histological definition of endometriosis). This discovery led to a biopsy of the lesion, the results of which confirmed the presence of intestinal endometriosis.
This case study serves to highlight how colonoscopy, when combined with other diagnostic methods like magnifying endoscopy and biopsy, can aid in the detection and diagnosis of bowel endometriosis.
The Future of Bowel Endometriosis Diagnosis
While the role and accuracy of colonoscopy in diagnosing bowel endometriosis have been explored, research in this area is ongoing. The development and refinement of diagnostic methods are crucial for improving the detection and treatment of bowel endometriosis.
In parallel with the innovations in medical technology, new diagnostic methods such as magnifying chromoendoscopy, target biopsy, and virtual colonoscopy are being explored and studied for their potential to improve the accuracy of bowel endometriosis diagnosis. These advancements, coupled with a deeper understanding of the condition, may pave the way for more accurate and less invasive diagnostic options in the future.
Bowel endometriosis is a complex condition that can significantly impact the quality of life of those affected. While colonoscopy can play a role in its diagnosis, its effectiveness and accuracy are subject to continuous research and improvement. Exploring new diagnostic methods and refining existing ones are crucial steps toward enhancing the detection and treatment of this condition. As we continue to learn more about bowel endometriosis and its nuances, we can hope for more efficient and accurate diagnostic tools in the future.
Related Reading:
- Endo-Fighting Microbiome Optimization: Research-based Tips
- Endometriosis and the Microbiome: Insights and Emerging Research
References:
- Walter SA, Kjellström L, Nyhlin H, Talley NJ, Agréus L. Assessment of normal bowel habits in the general adult population: the Popcol study. Scand J Gastroenterol. 2010;45(5):556-566. doi:10.3109/00365520903551332
- Habib, N., Centini, G., Lazzeri, L., Amoruso, N., El Khoury, L., Zupi, E., & Afors, K. (2020). Bowel Endometriosis: Current Perspectives on Diagnosis and Treatment. Int J Womens Health, 12, 35-47. https://doi.org/10.2147/IJWH.S190326
- Milone, M., Mollo, A., Musella, M., Maietta, P., Sosa Fernandez, L. M., Shatalova, O., Conforti, A., Barone, G., De Placido, G., & Milone, F. (2015). Role of colonoscopy in the diagnostic work-up of bowel endometriosis. World J Gastroenterol, 21(16), 4997-5001. https://doi.org/10.3748/wjg.v21.i16.4997
- Tomiguchi, J., Miyamoto, H., Ozono, K., Gushima, R., Shono, T., Naoe, H., Tanaka, M., Baba, H., Katabuchi, H., & Sasaki, Y. (2017). Preoperative Diagnosis of Intestinal Endometriosis by Magnifying Colonoscopy and Target Biopsy. Case Rep Gastroenterol, 11(2), 494-499. https://doi.org/10.1159/000475751

Through the Looking Glass: Reflecting on 2023
Embarking on the journey of self-reflection is not just a personal endeavor; for us at iCareBetter, it’s a collective celebration of progress, community, and collaboration. As we bid farewell to 2023, a year marked by challenges and triumphs, it’s time to take a look into the past year and reflect on all that has been accomplished. Join us as we navigate through the areas of growth, community involvement, projects, and meaningful collaborations that shaped our year. In this special blog post, we’re excited to share the insights gained from our podcast endeavors and offer a sneak peek into the thrilling developments that await us in 2024. Let’s rewind, recap, and anticipate the exciting narrative that continues to unfold in the ever-evolving story of iCareBetter.
About iCareBetter
iCareBetter is an innovative platform dedicated to helping patients with endometriosis and chronic pelvic pain find compassionate and skilled experts. All experts on iCareBetter have shown knowledge and expertise in the treatment of endometriosis and chronic pelvic pain.
Vision
Our vision is to reduce the symptom-to-effective treatment of endometriosis to less than a year. Studies show that patients with endometriosis spend an average of 7.5 years to have an official diagnosis. Moreover, even after the diagnosis, patients will have to spend several years with multiple failed treatment attempts. After the long delays in diagnosis and treatment, they might be lucky enough to receive effective treatment from an expert.
Mission
Our mission is to improve access to high-quality specialized care for those with endometriosis. iCareBetter wants to combat the issue of patients living in confusion, pain, and isolation. To that end, we hope to connect as many patients to the right experts as early as possible. And we hope that this will ensure timely diagnosis and effective treatment.
To read more about why iCareBetter was built and the inspiration behind it, check out our blog here and listen to episode 1 of the podcast here, where Saeid and Jandra give you a behind the scenes look into what inspired them.
What happened in 2023?
In 2023, iCareBetter grew in many ways, including new avenues to provide education along with collaboration from the community. Here are some of the highlights!
- We started a podcast! iCareBetter: Endometriosis Unplugged is hosted by Jandra Mueller, DPT, MS a pelvic floor physical therapist and endometriosis patient. The podcast is available on Spotify, Apple Podcasts, and Youtube.
- We had 19 weekly episodes in season one
- Listeners joined from all over the world, reaching 22 countries
- We brought on a team to help with new content on social media creating a more visually appealing platform, community engagement, and followers.
- We now have 211 providers on our website available and ready to help those suffering from endometriosis and we are continuing to grow!
- Our blog content is now consistent with twice weekly posts bringing you updates on all things endometriosis.
What To Expect in 2024
While 2023 was a big year for iCareBetter, we hope to continue the growth and expand our providers across the globe. Our hope is to increase our collaboration with medical specialists, researchers, and advocates. There are some exciting things to come in 2024 including a new season of iCareBetter: Endometriosis Unplugged as well as some other projects that will be announced in 2024.
We hope you have found our resources helpful either for yourself or a loved one, and hope you continue to share the love and spread the word about Endometriosis. All of us here at iCareBetter wish you a safe and happy new year.

Cheers to 2024!
Do you or a loved one have Endometriosis? Here are some blogs that may help you get started on your journey.
- Endometriosis Signs and Symptoms: Everything You Need to Know
- Endometriosis Facts & Myths: Dispelling the Misconceptions
Endometriosis and the Microbiome: Insights and Emerging Research
Table of contents
- Understanding Endometriosis
- The Human Microbiome and Its Role in Health and Disease
- The Microbiome-Endometriosis Connection: An Emerging Field of Research
- Microbiome and the Inflammatory Response in Endometriosis
- The Gut Microbiome and Estrogen Levels
- The Microbiome as a Diagnostic and Therapeutic Target
- Conclusion
Endometriosis is a multifaceted, heterogenous, inflammatory condition that impacts 10%-15% of women (XX) in their reproductive years, most commonly associated with chronic pelvic pain and infertility.
Over the years, numerous theories have been proposed to explain its pathogenesis, but none have conclusively clarified its origins. Recently, however, researchers have begun investigating the complex interplay between endometriosis and the human microbiome. This article aims to provide an in-depth exploration of the current research into the relationship between endometriosis and the microbiome, with a particular focus on gut health, inflammation, and pathogenesis.
Understanding Endometriosis
Endometriosis is marked by the growth of endometrial-like tissue found outside of the uterine cavity. This tissue is commonly found implanted over visceral and peritoneal surfaces within the abdominopelvic cavity, but can extend to the connective tissue and organs throughout the body. The condition can lead to severe dysmenorrhea, pelvic pain, and subfertility among a number of other symptoms and manifestations, significantly impairing a person’s quality of life.4
Read more: What causes endometriosis?
The Human Microbiome and Its Role in Health and Disease
The human microbiome comprises microorganisms that colonize our bodies and play crucial roles in nutrient metabolism and various physiological functions. The composition and balance of these microbial communities can significantly influence our health. For instance, the gut microbiota synthesizes vitamins B12 and K, maintains intestinal mucosal integrity, promotes angiogenesis and epithelial repair, and modulates immune functions.5
Disruptions in gut microbiota composition, a state known as dysbiosis, can contribute to the development and progression of numerous diseases, including inflammatory bowel diseases, arthritis, psoriasis, neuropsychiatric diseases, and even malignancies.4 Given that endometriosis is a chronic inflammatory disease potentially triggered by altered immune functions and increased angiogenesis, there is a growing interest in investigating the role of microbiota dysbiosis in the pathogenesis and pathophysiology of endometriosis.1,4
The Microbiome-Endometriosis Connection: An Emerging Field of Research
Recent studies have commenced exploring whether microbiome composition is altered in women with endometriosis. For instance, one study identified significant differences in the microbial community structure between those with and without endometriosis.1,5 This study found that the abundance of Acinetobacter, Pseudomonas, Streptococcus, and Enhydrobacter significantly increased, while the abundance of Propionibacterium, Actinomyces, and Rothia significantly decreased in the endometriosis group.5
Another study focused on the microbiota of extracellular vesicles in the peritoneal fluid.4,5 These vesicles, small structures made of bilayered lipid membranes released by cells, carry proteins, nucleic acids, and lipids, and play a key role in immune function, inflammatory reactions, and disease development. Like other cells, bacteria can release extracellular vesicles that modulate host-cell immune responses and other health conditions. The study found significant differences in the microbial community of these vesicles between women with and without endometriosis.5
Highlighting the complex relationship between the microbiome and endometriosis, several studies have shown an increased bacterial colonization of menstrual blood and endometrial tissue in women with endometriosis compared to control subjects.5 A study on rhesus monkeys demonstrated that altered composition of the intestinal microflora and intestinal inflammation are associated with endometriosis. While we know animal comparison is not exactly like humans, the reproductive tract of rhesus monkeys closely resembles humans in both the form and function.7
Read more: Endo-Fighting Microbiome Optimization: Research-based Tips
Microbiome and the Inflammatory Response in Endometriosis
Endometriosis is known to trigger an inflammatory response within the body, characterized by increased production of pro-inflammatory cytokines, autoantibodies, growth factors, oxidative stress, and alterations in T-cell and natural killer cell reactivity.1 This dysregulated immune response potentially creates an immunosuppressive environment that enables the growth of these endometriosis lesions.1
Recent studies suggest that gut microbiome-derived extracellular vesicles could play a critical role in this process.5 These vesicles, ranging from 20 to 400 nm in diameter, can traverse the intestinal barrier, enter the systemic circulation, and potentially influence the peritoneal environment. They may carry a cargo of proteins, nucleic acids, and lipids that can influence immune function, inflammatory responses, and the development of diseases like endometriosis.
One study demonstrated that extracellular vesicles from women with endometriosis carry unique cargo that can influence inflammation, angiogenesis, and proliferation.5 Another study identified specific proteins in the exosomes of peritoneal fluid samples from patients with endometriosis, suggesting a role of exosomes in the diagnosis and treatment of endometriosis.5
The Gut Microbiome and Estrogen Levels
The gut microbiome is a significant regulator of estrogen levels, influencing estrogen metabolism and hence potentially affecting estrogen-dependent diseases like endometriosis.3 In postmenopausal women, fecal microbiota richness and levels of fecal Clostridia taxa have been associated with systemic estrogen levels. Therefore, gut dysbiosis leading to abnormal circulating levels of estrogen could potentially play a role in the development of endometriosis or the associated symptoms.3
The Microbiome as a Diagnostic and Therapeutic Target
The alterations in microbiota composition associated with endometriosis may provide valuable diagnostic markers for the disease. For instance, one study has proposed a microbiota-based model that can distinguish infertile patients with and without endometriosis.1 Another study has found that specific bacterial species are enriched in the endometrium and peritoneal fluid of patients with endometriosis.2
On the therapeutic front, the modulation of gut microbiota through dietary interventions, prebiotics, probiotics, or fecal microbiota transplantation could potentially represent a novel treatment approach for endometriosis.4 However, more research is needed to explore the potential of these strategies and to understand the precise mechanisms through which the microbiota influences endometriosis development and progression.
Read More: Integrative Therapies for Endometriosis
Conclusion
The complex relationship between the microbiome and endometriosis is still in its early stages of investigation. Recent studies indicate that alterations in microbiota composition may be associated with endometriosis. These insights not only enhance our understanding of endometriosis pathogenesis but also open up new possibilities for the diagnosis and treatment of this prevalent condition.
As our understanding of the microbiome continues to grow, so does the potential for novel, integrative health strategies that target this complex ecosystem. Further research is required to confirm the observed associations and to elucidate the mechanisms underlying the microbiome-endometriosis connection. Such research holds the promise of ushering in a new era in our approach to endometriosis, one that acknowledges the intricate interplay between our bodies and the microbes that inhabit them.
While there are limitations in the current usefulness of this research, we do know that the immune system is involved with regulating the disease. An important question remains: are the microbiota changes seen in those with endo the chicken or the egg?
References:
- Leonardi, M., Hicks, C., El-Assaad, F., El-Omar, E., & Condous, G. (2020). Endometriosis and the microbiome: a systematic review. BJOG, 127(2), 239-249. https://doi.org/10.1111/1471-0528.15916
- Oishi, S., Mekaru, K., Tanaka, S. E., Arai, W., Ashikawa, K., Sakuraba, Y., Nishioka, M., Nakamura, R., Miyagi, M., Akamine, K., & Aoki, Y. (2022). Microbiome analysis in women with endometriosis: Does a microbiome exist in peritoneal fluid and ovarian cystic fluid? Reprod Med Biol, 21(1), e12441. https://doi.org/10.1002/rmb2.12441
- Svensson, A., Brunkwall, L., Roth, B., Orho-Melander, M., & Ohlsson, B. (2021). Associations Between Endometriosis and Gut Microbiota. Reprod Sci, 28(8), 2367-2377. https://doi.org/10.1007/s43032-021-00506-5
- Jiang, I., Yong, P. J., Allaire, C., & Bedaiwy, M. A. (2021). Intricate Connections between the Microbiota and Endometriosis. Int J Mol Sci, 22(11). https://doi.org/10.3390/ijms22115644
- Lee, S. R., Lee, J. C., Kim, S. H., Oh, Y. S., Chae, H. D., Seo, H., Kang, C. S., & Shin, T. S. (2021). Altered Composition of Microbiota in Women with Ovarian Endometrioma: Microbiome Analyses of Extracellular Vesicles in the Peritoneal Fluid. Int J Mol Sci, 22(9). https://doi.org/10.3390/ijms22094608
- Wei, W., Zhang, X., Tang, H., Zeng, L., & Wu, R. (2020). Microbiota composition and distribution along the female reproductive tract of women with endometriosis. Ann Clin Microbiol Antimicrob, 19(1), 15. https://doi.org/10.1186/s12941-020-00356-0
- Burns, K. A., Pearson, A. M., Slack, J. L., Por, E. D., Scribner, A. N., Eti, N. A., & Burney, R. O. (2021). Endometriosis in the Mouse: Challenges and Progress Toward a ‘Best Fit’ Murine Model. Front Physiol, 12, 806574. https://doi.org/10.3389/fphys.2021.806574

Navigating the Path to Your Best Endometriosis Specialist
The journey towards resolving endometriosis involves an important decision – selecting the best endometriosis specialist.
Table of contents
Determining Your Needs in a Surgeon
Being aware of your specific requirements can help you make an informed choice. Here are a few considerations you should keep in mind:
Training and Experience
A surgeon’s training, notably in Minimally Invasive Gynecologic Surgery (MIGS) or Fellowship in Minimally Invasive Gynecologic Surgery (FMIGS) is crucial. Such surgeons have spent more time in operation theaters, honing their skills through extensive practice.
Ensure your surgeon is board-certified and inquire about their experience, including the number of surgeries they’ve performed, complications they’ve encountered, and outcomes.
Surgical Support Team
The surgeon’s team is equally important. Ask about their procedure in case of bowel, bladder, ureter, or diaphragmatic involvement. Inquire if everything can be done during a single procedure.
Approach to Excision
Surgeons may have different opinions on excision versus ablation. Find out their thoughts on the subject and where and when they excise or ablate.
Post-Surgery Care
Ask if the surgeon routinely prescribes suppressive medications pre and post-surgery. Understand their reasons if they do.
Costs
Don’t hesitate to inquire about costs, insurance acceptance, payment policies, and any hidden charges.
Comfort Level
Ensure you feel comfortable conversing with your surgeon and that your queries are answered satisfactorily.
Factors That May Not Influence Your Decision
Certain aspects may not influence the quality of surgical care:
- Gender: The surgeon’s gender does not impact their surgical ability.
- Preferred Tools: The surgical tool used is less important than the surgeon’s skill.
- Bowel Prep: Surgeons may have different preferences for bowel prep before surgery, but it doesn’t seem to influence the outcome.
Factors That Might Influence Your Decision
Some factors might play a role in your decision-making process:
- Reputation: Be cautious while considering a surgeon’s reputation. Some may get media coverage or have excellent bedside manners, but that doesn’t necessarily make them a skilled surgeon.
- Office Management: A well-managed front office can make your experience smoother.
- Location: Depending on your comfort and ability to travel, location might influence your decision.
- Timing: The availability of the surgeon and your urgency might also play a role.
The Most Important Factor
Patients often report being most satisfied with surgeons who actively listen to them. Your surgeon should respect your knowledge and experiences without objection to being recorded or having someone with you during consultations.
Leading Endometriosis Specialists
iCareBetter has a list of endometriosis specialists and surgeons vetted for their surgical skills.
Managing Your Relationship with Your Current Doctor
Dealing with a current doctor who might not be capable of handling your endometriosis can be challenging. Here are some tips:
- Think long-term, maintain a cordial relationship, and educate your doctor about your condition without alienating them.
- Be respectful and considerate of your doctor’s opinions.
- Try to keep your doctor on your side by asking for their support.
- Remain calm and collected during discussions.
- If you choose to seek surgery elsewhere and decide not to return to your current physician, send a copy of the operative and pathology reports with a note of gratitude.
- If your doctor dismisses you as a patient, consider it as a sign that it wasn’t a good fit.
- Routine care can be handled by a GP or Family Doctor, a Nurse Practitioner, or a Physician’s Assistant.

Interstitial Cystitis and Endometriosis: Unraveling the Evil Twins Syndrome of Chronic Pelvic Pain
Table of contents
Introduction
Chronic pelvic pain (CPP) is a health condition that burdens millions of women worldwide. The complexity of diagnosing and treating CPP is often overwhelming due to the multitude of potential underlying causes and associated conditions. Two such conditions, often called the “Evil Twins” syndrome, are Interstitial Cystitis (IC) and Endometriosis, both commonly found in patients suffering from CPP. This article will explore these conditions’ prevalence, diagnosis, and treatment in patients with CPP.
Understanding Chronic Pelvic Pain
Chronic Pelvic Pain (CPP) is a prevalent health condition affecting an estimated 9 million women in the United States alone. It accounts for up to 40% of laparoscopies and 10% to 12% of all hysterectomies, indicating its significant impact on women’s health. The annual expenditure on diagnosing and treating CPP is nearly $3 billion.
The “Evil Twins”: Interstitial Cystitis and Endometriosis
Two conditions frequently associated with CPP are Interstitial Cystitis (IC) and Endometriosis. These conditions can present similar symptoms and coexist in patients, making the diagnosis and management of CPP even more challenging.
Interstitial Cystitis (IC)
Interstitial Cystitis, or bladder-originated pelvic pain, is a significant disorder related to CPP. The etiology of IC is multifactorial and progressive, involving bladder epithelial dysfunction, mast cell activation, and bladder sensory nerve upregulation. The exact prevalence of IC in the United States varies, with estimates ranging from 10 to 510 per 100,000 normal population. However, current research suggests that IC might be more prevalent than previously estimated.
Endometriosis
Endometriosis is another common condition among women with CPP, affecting more than half of the patients diagnosed with CPP. Symptoms include pain during sexual intercourse (dyspareunia), cyclical perimenstrual lower abdominal pelvic pain, symptom flares after sexual intimacy, and irritative voiding in case of urinary tract involvement. A definitive diagnosis of endometriosis requires visual confirmation of the lesion during laparoscopy and histologic confirmation of the presence of both ectopic endometrial glands and stroma.
The Overlap Between Interstitial Cystitis and Endometriosis
Research has demonstrated a high rate of overlap between IC and endometriosis in patients with CPP. This overlap poses challenges in diagnosis and treatment, as the presence of one condition does not preclude the existence of the other. Therefore, it is crucial to consider both conditions in the evaluation of patients with CPP.
Diagnosis of Interstitial Cystitis
The diagnosis of IC and endometriosis involves various tests and procedures, including the Potassium Sensitivity Test (PST), cystoscopy with hydrodistention, and laparoscopy.
Laparoscopy
Laparoscopy for direct visualization of endometriosis lesions and taking a biopsy is the gold standard for endometriosis diagnosis.
Read more: The Different Tests Used to Diagnose Endometriosis
Potassium Sensitivity Test (PST)
The PST is a diagnostic test developed to detect abnormal permeability of the bladder epithelium, a key factor in the pathophysiology of IC. Previous studies have validated the use of the PST in diagnosing IC, particularly at the early stages of the disease.
Cystoscopy with Hydrodistention
Cystoscopy with hydrodistention is a diagnostic procedure often used to confirm the presence of IC. The bladder is filled with sterile water under passive hydrostatic pressure, then slowly drained. The presence of submucosal petechial hemorrhages, or glomerulations, confirms the diagnosis of IC.
Biopsy
During cystoscopy under anesthesia, your provider may remove a sample of tissue (biopsy) from the bladder and the urethra for examination under a microscope. This is to check for bladder cancer and other rare causes of bladder pain.
Urine cytology
Your provider collects a urine sample and examines the cells to help rule out cancer.
Conclusion
This article highlights the complex interplay between IC and endometriosis in the context of CPP. It underscores the need for careful evaluation and simultaneous consideration of these conditions in patients with CPP. A multidisciplinary approach, including the use of PST and concurrent cystoscopy and laparoscopy, is crucial for accurate diagnosis and effective treatment of concurrent interstitial cystitis and endometriosis.

Endo-Fighting Microbiome Optimization: Research-based Tips
Table of contents
Endometriosis is partly caused by, and causes, inflammation. The origin or genesis of this
inflammation is probably multifactorial but recent research suggests that the microbiome, the
community of microorganisms living in or on the human body, plays an important role through
inflammatory pathways. Dysbiosis, which means an imbalance or impairment of the microbiota,
is observed in endometriosis, and is thought to both contribute to and result from endo.
Studies have focused on the gut, peritoneal fluid, and female reproductive tract microbiota to
identify specific microbiome signatures associated with endometriosis. The gut microbiome, in
particular, has been extensively studied. Changes in bacterial composition, such as increased
levels of Proteobacteria and decreased levels of Lactobacilli, have been observed in the gut of
endometriosis patients. Other body sites, including the peritoneal fluid and female reproductive
tract, also show altered microbiota in endometriosis.
The dysbiosis observed in endometriosis is believed to contribute to the disease through
various mechanisms. One theory suggests that bacterial contamination, particularly with
Escherichia coli, in the menstrual blood may lead to inflammation and immune activation in the
peritoneal cavity, contributing to endometriosis development. Dysbiosis can also affect
estrogen metabolism, through dysfunction of the so called “estrobolome”. This can lead to
increased levels of circulating estrogen and a hyper-estrogenic state, which promotes
endometriosis. Additionally, dysbiosis-induced epigenetic changes and immune modulation
may play a role in direct endometriosis pathogenesis.
Research on the microbiome in endometriosis is still in its early stages, but it holds promise for
potential diagnostic and therapeutic approaches. Microbiome testing could potentially be used
as a non-invasive tool for detecting endometriosis, complementing current imaging modalities.
The technology for doing this is already here and you can get it ordered. However, the meaning
of the results is still not well understood in any given individual. So, it’s complicated.
Beyond testing, manipulating the microbiome through interventions like probiotics, antibiotics,
or dietary modifications may offer new treatment options for endometriosis. To the extent that
you can diversify your microbiome and get it to a healthier state, this is something that can be
done with little risk or cost today. Options available to you are covered below, most of which
are focused on the bacterial part of your microbiome.
Future studies will explore the role of different types of microorganisms, beyond bacteria, such
as viruses and fungi, and utilize advanced analytical methods like shotgun metagenomics and
metabolomics to gain a more comprehensive understanding of the microbiome in
endometriosis. Newer technologies like this are significantly accelerating gains in knowledge.
Meanwhile, emerging understanding of the bidirectional relationship between endometriosis
and the microbiome has implications for potential treatment strategies available today.
Antibiotics
Antibiotics could be used to target specific bacteria associated with dysbiosis in
endometriosis, especially if you are diagnosed with small intestinal bacterial overgrowth (SIBO).
Animal studies have shown that treatment with antibiotics can reduce the size of endometriotic
lesions and associated inflammation. In humans, we know that chronic endometritis (infection
of the uterine cavity) seems to play a role in development of endo. However, this requires
expert guidance. It’s critical to exercise caution with antibiotic use to avoid disrupting healthy
commensal (good bacteria) microbiota and contributing to antimicrobial resistance. You don’t
want to grow a bug that might be resistant to multiple antibiotics down the line.
Probiotics
Probiotics are live bacteria that can have beneficial effects on your microbiome
health and diversity when consumed. Studies in animal models have demonstrated that certain
probiotic strains, such as Lactobacillus gasseri, can suppress the development and growth of
endometriotic lesions. Probiotics may modulate the immune response and restore a healthier
microbiota composition, potentially mitigating the inflammatory processes associated with
endometriosis. However, again, this requires expert guidance because, for example, it could
lead to ineffectiveness against or exacerbation of SIBO. This is partly because there are at least
three different general types of SIBO, based on what type of gas is produced by the
microbiome.
Prebiotics
Prebiotics are basically food substances that selectively promote the growth of
beneficial bacteria in the gut. By providing a favorable environment for beneficial bacteria,
prebiotics can help restore a healthy microbiota balance. An example of a prebiotic shown to
be beneficial in SIBO treatment is partially hydrolyzed guar gum (PHGG). Further research is
needed to investigate the potential roles of prebiotics in endometriosis treatment, but it could
be a gamechanger for simple treatment of various intestinal disorders, leaky gut and so on.
Dietary Modifications
Diet can hugely influence the composition and activity of the
microbiome. Consuming a diet rich in fiber and plant-based foods, which are known to support
a diverse and healthy microbiota, may have beneficial effects on endometriosis. Low FODMAPs
diets, which restrict fermentable carbs, can help. Omega-3 polyunsaturated fatty acids (PUFAs),
found in fatty fish, flaxseeds, and chia seeds, have shown anti-inflammatory properties and
have been associated with a lower incidence of endometriosis. Incorporating these dietary
changes, among many others, may help modulate the microbiome and reduce inflammation.
Immunomodulation
The microbiome has profound effects on the immune system, and
targeting the immune response could be a potential avenue for endometriosis treatment.
Modulating the immune system through therapies such as immune-suppressing medications or
immune-modulating agents may help regulate the inflammatory processes associated with
endometriosis. The idea here is to keep it as natural as possible, but sometimes prescription
medications may turn out to be necessary.
Please keep in mind that these treatment implications are based on current research, primarily
in the lab and animal models, and further studies are needed to validate their effectiveness and
safety in humans. Additionally, personalized approaches considering an individual’s specific
microbiota composition and disease characteristics may be necessary for optimal treatment
outcomes. It is exciting research in development and will be part of upcoming revolutionary
advances which take us far beyond hormonal manipulation for endo management. Since these
approaches are exploring the root cause of endo, treatments will likely be therapeutic as
opposed to simply something that reduces symptoms, which is the case with today’s hormonal
therapies.
The best part is that with proper expert guidance, much of the above can be used today
because, in most cases, the risk and cost are relatively low.
References:
Uzuner, C., Mak, J., El-Assaad, F., & Condous, G. (2023). The bidirectional relationship between
endometriosis and microbiome. Frontiers in Endocrinology, 14, 1110824. doi:
10.3389/fendo.2023.1110824
Moreno, I., Franasiak, J. M., & Endometrial Microbiome Consortium. (2020). Endometrial
microbiota—new player in town. Fertility and Sterility, 113(2), 303-304. doi:
10.1016/j.fertnstert.2019.10.031

How Do Endo Fertility Issues Impact the Mental Health of a Person?
Table of contents
- Why Are Women Impacted Emotionally By Reproductive Disorders?
- Endometriosis Patients with Fertility Issues Need Emotional Support
- All Endometriosis Patients Could Benefit From Emotional Support
- Seeking a Mental Health Provider Experienced With Endometriosis
- Importance of Friends and Family
- Do You Have Fertility Issues Caused By Endometriosis?
Endometriosis (endo) can cause many issues. Endometriosis patients may have difficulty becoming pregnant or maintaining a full-term pregnancy. Up to 70% of women with endometriosis get pregnant without medical treatment. However, 30 to 50% of patients with endo experience fertility issues and may need endometriosis fertility treatments or surgery. Up to 50% of all women with infertility have endometriosis. According to the abstract in a study published in the International Journal of Women’s Health:
“The most common clinical signs of endometriosis are menstrual irregularities, chronic pelvic pain (CPP), dysmenorrhea, dyspareunia and infertility. Symptoms of endometriosis often affect psychological and social functioning of patients. For this reason, endometriosis is considered as a disabling condition that may significantly compromise social relationships, sexuality and mental health.”
Why Are Women Impacted Emotionally By Reproductive Disorders?
A plethora of reasons exists as to why women can experience deep emotional impact by a diagnosis of a reproductive disorder or a condition that could cause issues with fertility. Some women already worry about getting pregnant anyway, so an endometriosis diagnosis surely doesn’t help. Here’s a shortlist of some reasons reproductive issues can affect the emotional health of women with endometriosis:
- Pressure to conceive right away
- Worries about each stage of the pregnancy, from implantation to delivery
- Pressured to have a child, even if the person is unsure or not ready
- Possible medical interventions, such as IVF
- Stress and emotional drainage that can result from endometriosis fertility treatments
- Possible laparoscopy endometriosis surgery
Multiple studies demonstrate that a woman’s ability to conceive and bear a child plays a big part in her emotional health and self-esteem. While many women don’t want to have children, a large portion does. But, they might not be ready for a baby when they receive their endometriosis diagnosis. According to a study out of the Iranian Journal of Reproductive Medicine:
“While infertility is not a disease, it and its treatment can affect all aspects of people’s lives, which can cause various psychological-emotional disorders or consequences including turmoil, frustration, depression, anxiety, hopelessness, guilt, and feelings of worthlessness in life.”
Endometriosis Patients with Fertility Issues Need Emotional Support
Most endometriosis patients with fertility issues benefit by having a mental health provider as part of their multidisciplinary team.
Endometriosis impacts many facets of a person’s life. A recent study concluded that:
“Furthermore, there is an urgent need to develop and evaluate interventions for supporting women and partners living with this chronic and often debilitating condition.”
All Endometriosis Patients Could Benefit From Emotional Support
Many endometriosis patients with fertility issues express no desire to have children. Therefore, some women are unaffected by infertility that might arise from endo. However, it’s essential to keep these women in mind because their feelings matter, too. Perhaps some did not want to have kids now but were hoping to someday in the future? Or maybe they are just not with the right person to have children with them?
Whatever the case may be, it’s significant that healthcare providers do not overlook a patient’s emotional needs, even if they say it doesn’t bother them if they cannot have kids. Perhaps a person in this situation may not need as intense emotional support, but they should see a mental health provider have a chance to talk about these feelings and think them through. Some interventions can help one conceive or be ready to conceive even with an endometriosis diagnosis. However, it’s significant to remember that the further the disease has progressed, the more complex it is to treat it to regain fertility. Therefore, when you are unsure if you want to have a baby, it’s still wise to have all the lesions removed as soon as you can and conduct proper follow-up.
Seeking a Mental Health Provider Experienced With Endometriosis
Endometriosis is a complex and often misunderstood disease. Therefore, women who battle this condition daily, especially those with fertility issues, require a mental health professional familiar with this inflammatory disorder.
Endometriosis encompasses many domains of a patient’s life, and fertility issues are not the only things that impact women’s emotional health. When seeking out a professional, it’s critical to find someone familiar with the disease and its emotional impact on patients.
Importance of Friends and Family
In addition to adding a robust mental health provider to your team, it’s also essential that you seek support from your loved ones. Please encourage them to attend appointments with you to have a better understanding of the condition. When the people closest to you can comprehend the emotional roller-coaster accompanying infertility, they will be better prepared to support you emotionally.
When a patient receives a diagnosis such as endometriosis, pain management, and other care items often become the priority. Therefore, it can be easy to overlook the emotional aspect of this condition, especially in someone with fertility issues. This is why it’s essential to do your research and find an experienced endometriosis expert to head up your team.
Do You Have Fertility Issues Caused By Endometriosis?
We want to hear from you. What are your thoughts on the emotional challenges? Do you have a solid mental health provider on your team? Leave your responses in the comments below.

Endometriosis and Fertility: Statistics, Facts, & Fiction
Table of contents
Debunking the Myths Surrounding Endometriosis and Reproduction
Disinformation about endometriosis and how it can impact reproduction is thick. As a matter of fact, not just endometriosis and fertility, the entire disorder is shrouded in junk information, and so it often goes misunderstood and mistreated. To learn more on this topic, read our previous article, titled: “Endometriosis Facts and Myths: Dispelling the Misconceptions.”
Does endometriosis cause infertility? In some cases, yes. However, in most cases, women with endometriosis can and do get pregnant without any medical assistance or intervention of any kind. There is still a myth that if you become pregnant, that can manage the endometriosis (endo) symptoms and even help resolve disease progression.
This statement couldn’t be further from the truth, and it’s an example of a widespread myth about endometriosis and fertility. Furthermore, this school of thought can put additional pressure on women with endometriosis to get pregnant as quickly as possible once they get a diagnosis. As you can imagine, this dangerous misinformation can alter their expectations in terms of treatment for fertility and their outlook on endometriosis in general.
So, Can You Get Pregnant If You Have Endometriosis?
The real truth is that the connection between endometriosis and reproduction is complex. Can you get pregnant if you have endometriosis? Yes, many people can and do. However, having the right endometriosis specialist to help you along the way can make all the difference in your journey. Click here to learn more about finding vetted endo specialists near you. In this article, we will review the disease and lay out the facts regarding endometriosis and fertility.
What is Endometriosis?
Endometriosis is an inflammatory disorder in which tissue similar to the uterus lining grows in places outside the uterus. Often these growths happen on the surface of the uterus, ovaries, fallopian tubes, or other organs within the pelvic cavity – such as the bladder or bowel. In some cases, these endometriosis growths have occurred in distant organs.
Endo growths can cause pain, scarring, and sometimes infertility. Because this tissue is similar to the uterine lining, it also bleeds and sheds once a month during hormonal changes. Typically in the uterus, this period tissue and blood have a means of escaping through the vagina. However, this blood and tissue often accumulate inside the body with endometriosis and causes inflammation and pain. As one can imagine, over time, scar tissue growths with subsequent menstrual cycles develop. Eventually, this scar tissue can fuse organs, immobilize organs, and even damage the fallopian tubes.
Alarming Statistics About Endometriosis & Fertility
- Endometriosis is widespread, affecting between six and ten percent of the general female population. That’s more than 170 million worldwide.
- In patients with pelvic pain, infertility, or both, endometriosis frequency is higher – between 35 percent to 50 percent.
- Between 25 percent to 50 percent of infertile women have endometriosis.
- Between 30 percent to 50 percent of women with endometriosis are infertile.
- Endometriosis affects approximately the same number of women around the world that have diabetes.
- The cost of endometriosis in the US is between $86 Bn – $116 Bn.
- It takes, on average, eight years from the onset of symptoms for a patient to get a diagnosis. This can impact all patients, but especially those of who wish to keep their fertility intact.
Endometriosis Facts About Fertility and Reproduction
- There are ways to get pregnant with endometriosis.
- Hormonal therapy does not cure endo.
- Endometriosis is related to your menstrual cycle and hormonal changes within your body.
- Endometriosis tissue can be removed during laparoscopy. Depending on the location of the growths and the extent of damage, this can sometimes restore fertility.
- There is a type of endometriosis that can cause cancerous lesions, typically dark chocolate brown.
- The causes are uncertain, and there is no “cure” for endometriosis.
- Genes seem to play a role in the occurrence of endo.
Myths About Endometriosis and Fertility
- Pregnancy is not a cure or a way to relieve symptoms of endometriosis. Women should not be pressured or encouraged to get pregnant to help with endometriosis and fertility or alleviate pain or other symptoms. While some women experience less endo pain and symptoms during their period, that does not mean it works the same for all women.
- Do not believe any physician that tells you a hysterectomy is the “gold standard” treatment for endometriosis. As mentioned above, there is no “cure” for endometriosis. Until a specialist is inside the body and can view the number and the placement of the endometriosis lesions, they cannot decide whether a hysterectomy would even solve the problems. Also, some women might make themselves infertile (whether they mind or not, it is an emotional part of this disorder) by having a hysterectomy done that was never needed.
- You do not need to have a major medical procedure to get an endometriosis diagnosis or remove some growths and lesions. With modern equipment, skilled specialists, and advanced technology (often robotic surgical equipment), you can have endometriosis diagnosis and treatment with laparoscopy. This type of procedure is minimally invasive and only leaves behind a few puncture wounds.
- Abortion does not cause endometriosis.
- Endometriosis does not cause ovarian cancer. Although a type of endo involves cancerous tumors, this does not mean that having endometriosis makes you more likely to develop cancer.
- The most important myth to bust is that there is no treatment for endometriosis. Just because there is no “cure” for this pelvic inflammatory disorder does not mean there are no treatment options, even when it comes to endometriosis and infertility.
If you have endometriosis, what is the most common thing you have heard regarding endo and reproduction?

Find Endometriosis Specialists for the Best Possible Outcomes
Table of contents
Why You Need an OB-GYN Who Specializes in Endometriosis
Endometriosis is common (affecting nearly 190 million women worldwide) but poorly understood by many medical professionals. It’s hard to find endometriosis specialists who have completed advanced training. With the proper endo specialist, medical treatment or surgery can lessen your pain, improve your quality of life, and manage complications.
Endometriosis is a chronic pain condition that affects 10-15% of women of reproductive age. It causes painful periods, bleeding between periods, pain during sexual intercourse, and discomfort when passing urine or feces. Despite causing chronic pelvic pain, many medical professionals have a poor understanding of the condition.
In this article, we will look into what endometriosis is and explore how to improve diagnosis, treatment, and outcome factors.
What is Endometriosis?
Endometriosis affects menstruating women and girls and some women post-hysterectomy or post-menopause. The condition also can affect transgender men and non-binary individuals. Endometriosis affects roughly 190 million people worldwide, with immune, genetic and hormonal factors all likely to be at play.
To understand Endometriosis, we first need to understand the endometrium or lining of the uterus.
The Endometrium
A large proportion of the endometrium is stromal cells. Stromal cells regulate cell growth and change during the menstrual cycle.
Endometrial glands line the endometrium. During the menstrual cycle, they widen in response to greater blood flow.
Each cycle, stromal cells, and endometrial glands slough off as part of menstruation.
Endometriosis Lesions
The presence of endometrium-like cells found outside the uterus causes the classic endometriosis symptoms. Discourse exists, but scientists have concluded a genetic basis to the cells’ presence, with endometrium-like cells migrating inappropriately during embryogenesis.
Endometriotic lesions can be in the ovaries, uterine ligaments, fallopian tubes, and pouch of Douglas (the space between the uterus and rectum). In some, lesions are present outside the pelvic cavity. Locations include the bowel, urinary tract wall, diaphragm, lungs, abdomen, and pericardium (the sack around the heart).
The endometrial-like tissue responds to the natural cycle of hormones and also produces some hormones by itself. This tissue has cycles of growth and bleeding.
Whereas menstrual blood in the uterus leaves the body via the vagina, the blood and tissues cannot escape from endometriosis lesions. This trapped cells and tissue leads to the painful processes of inflammation, adhesions, and scarring.
What does it feel like to have Endometriosis?
Although pain is the most common complaint, Endometriosis causes a wide range of symptoms, including:
- Painful periods
- Heavy periods (menorrhagia)
- Vaginal bleeding between periods
- Pain on passing urine or feces
- Bowel symptoms include bloating, constipation, diarrhea, or bleeding from the bowel
- Pain during intercourse
- Tiredness
- Depression
- Infertility.
Social and Emotional Effects
Severe pain can interrupt daily life for many patients. This interruption may include missing school, taking days off work, or being unable to socialize. A study in 2020 found that in over half of women, the pain had reduced their professional, physical, and sexual activity.
Endometriosis is associated with low mood. 15% of women are diagnosed with depression, with an average age at diagnosis of 22.
Infertility
Infertility can be the only symptom of Endometriosis for some women. Around 30-50% of patients cannot get pregnant owing to inflammation, pelvic adhesions, blockage of the fallopian tubes, and changes to the pelvic anatomy.
Other Symptoms
Additional symptoms are dependent on the location of endometriosis lesions. For example, an endometriotic lesion in the lung could cause breathlessness or chest pain. A study of over 2000 patients found that endometriotic nodules caused leg and buttock pain, as well as numbness, similar to sciatic pain.
Misdiagnosis and incorrect management are therefore common for women with symptoms that are not classic to pelvic endometriotic lesions.
Endometriosis Myths
The average delay in the diagnosis of Endometriosis is more than seven years, leading to “unnecessary suffering and reduced quality of life.” This delay leads many people to the internet to conduct their own research before and during diagnosis. However, the internet is awash with myths.
The importance of educating yourself via a reputable source such as iCareBetter cannot be understated.
Find Endometriosis Specialists for Appropriate Diagnosis & Treatment
The widespread misunderstanding of Endometriosis hinders its diagnosis and treatment. The inappropriate investigation, treatment with analgesics, or hormonal suppression do little to manage the cause while delaying diagnosis. Women who felt they were not listened to nor understood by doctors have described frustration, anger, annoyance, and sadness.
Reassuringly, appropriate diagnosis and treatment can lead to significant improvements in pain. This is precisely why it is crucial to find an endometriosis specialist. Only highly specialized surgeons with a comprehensive team can perform a thorough excision to remove endometriotic lesions, including extra-pelvic locations. Complete removal can significantly improve overall outcomes, including relief from pain and increased quality of life.
iCareBetter Endometriosis Care
iCareBetter is a platform that connects patients with experts in endometriosis care. At iCareBetter, patients have access to surgeons who have completed advanced training. These professionals have shown expertise in the diagnosis and treatment of complex Endometriosis. iCareBetter utilizes a transparent and unbiased system to ensure that only doctors with proven advanced excision skills and a comprehensive care team can be on their surgeons’ list.
Patients can select their surgeon based on their specific symptoms. This empowers patients to consult a doctor who truly understands the complexity of their condition. Patients can access specialists for endometriosis in the pelvis, bowels, bladder, thorax, heart, or diaphragm. They also can find help with infertility issues.
A highly specialized endo surgeon will take a holistic approach to treatment. This holistic approach includes managing secondary comorbidities such as infertility, even in stage III and IV disease patients.
At iCareBetter, patients can also access expert physical therapists who understand the condition. Working with a physical therapist gives access to myofascial release techniques, visceral mobilization, and the tools to manage a susceptible nervous system for better pain management.
Team-based expert care improves post-operative outcomes. For some iCareBetter doctors, post-treatment reports of satisfactory pain relief could be over 80%, with less than 20% of women requiring subsequent pelvic surgery. Moreover, many patients see reduced pain relief requirements post-recovery.
Standards of excellence, such as those endorsed by iCareBetter, must become a driving force behind treatment protocols for Endometriosis. Women should no longer shoulder the pain and reduced quality of life associated with substandard care.
Conclusion
Endometriosis occurs due to the presence of endometrium-like cells found outside the uterus. The resulting inflammation, adhesions, and scarring can cause severe pain and symptoms related to the location of the lesions. By connecting patients with expert surgeons in endometriosis care, iCareBetter empowers patients to access the care leading to better outcomes. Advanced surgical excision, physical therapy, and an expert team-based approach can reduce pain, as well as skillfully manage secondary complications.
Find endometriosis specialists today.

Impact of Living with Endometriosis and Mental Health
(All research studies mentioned in this article about the impact of endometriosis on mental health enrolled people with assigned female gender at birth. However, to be inclusive to all people with endo, we use people throughout the article.)
Being diagnosed with endometriosis (endo) and living with it can bring up a lot of emotions. It can mean making space for changes that you may never have predicted or accounted for. Endometriosis impacts nearly 200 million people worldwide, but there is pernicious misinformation and a lack of awareness and understanding among the medical community and the larger society. This misinformation and lack of awareness stand in the way of receiving a timely diagnosis.
It takes, on average, over seven years for a person who has endometriosis to get a diagnosis. Essentially, this means experiencing intense pain, feeling unheard over and over, and being gaslit at a systemic level for at least seven years.
In most countries, managing the pain and heavy periods remain the first line of treatment for endometriosis. If one is lucky, they can access endometriosis excision surgery. However, the impact of endometriosis goes beyond just the physical. The effect of endometriosis on mental health and the emotional wellbeing of the person is enormous.
Link Between Endometriosis Pain and Mental Health
The mental health struggles of living with endometriosis vary from person to person. The debilitating chronic endometriosis pain, one of the most common symptoms, is a critical factor that impacts the quality of life and mental health. Along with the cyclic pelvic pain, one may also experience other types of pain in varying degrees:
- Non-menstrual pelvic pain
- Pain during ovulation, urination, and/or bowel movements
- Pain during sex
- Sciatic pain
- Pain post and during orgasms
- Widespread full-body pain.
Research published in the International Journal of Women’s Health Health looked at the link between common symptoms of endometriosis and mental wellbeing.
It found that a person experiencing chronic pelvic pain (CPP) is likely to feel higher levels of anxiety and depression, which can further amplify the perception and severity of pain, thus placing them in a vicious circle of physical and psychological distress.
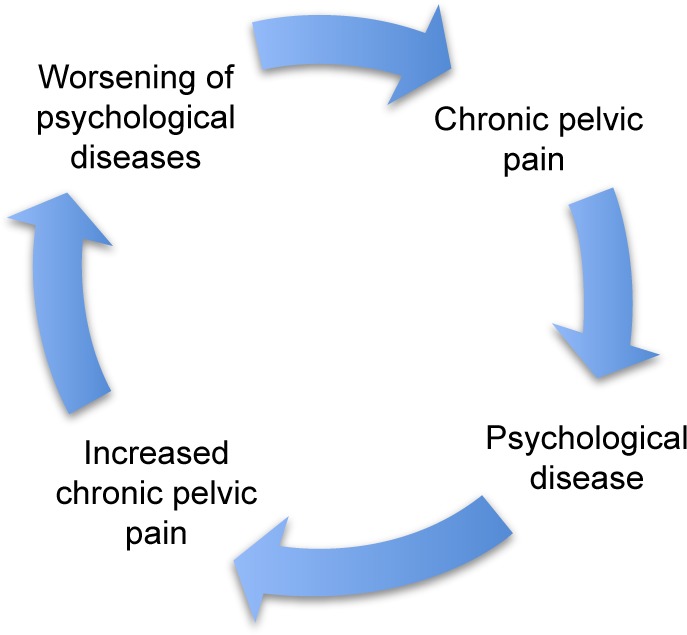
Figure 1: The vicious circle of chronic pelvic pain and psychological disease.
Pelvic Pain Causes Further Effects of Endometriosis on Mental Health
A study found that endometriosis patients with pelvic pain had poorer quality of life and mental health than those with asymptomatic endometriosis. It also showed that non-menstrual pelvic pain impacts all the variables of a person’s life. Thus, the study emphasized psychological interventions as an essential aspect of the endometriosis treatment plan and pain management treatments and interventions.
In another meta-analysis of 99,614 people from 24 different studies, researchers found that chronic pelvic pain was a primary factor contributing to the higher rates of depression in patients with endometriosis. This study emphasized that treating this kind of depression with antidepressants without the efforts towards managing the chronic pain would indeed be ineffective.
The Emotional Reality of Endometriosis
Studies have tried to understand the impact and management of endometriosis within the medical healthcare system. But still, the health system has largely overlooked the effect of endometriosis on mental health.
Living with endometriosis can make daily activities a struggle, mainly due to the unpredictability of pain and fatigue. The struggle makes some tasks nearly impossible. These tasks can include planning, working, socializing, exercising, eating, or even basics like cooking, cleaning, and bathing. This inability fuels guilt and anxiety. Furthermore, the debilitating pain being reduced to “just a bad period” or “psychosomatic” often leaves one feeling gaslit, isolated, depressed, and sometimes suicidal.
This distress increases due to the lack of systemic and psychosocial support. When the BBC spoke to 13,500 people (female assigned at birth) with endometriosis, more than 50% of the respondents felt suicidal ideations.
This is a battle
For someone living with chronic pain every day, even a short-lived moment of low pain brings ease, which allows one to hope for a future not controlled by pain. However, grief sets in quickly as fatigue and flare-ups follow. These changes make life with endometriosis incoherent and an inescapable dance between hope and grief. A Swedish study concluded that people living with painful endometriosis underwent a constant struggle for coherence in their lives. It emphasized that healthcare providers should validate this struggle by understanding the disease-related grief.
The anxiety around pain and health, the grief related to the future, the loneliness and isolation often bring up the feeling that chronic pain has monopolized one’s life. Endometriosis becomes the central point around which all decisions revolve. It takes away the body’s ability to be reliable and the capacity to feel safe within it. It often changes the way one views themselves and takes the world in.
One of the ways we feel safe in the world is by feeling safe in our bodies. Then what happens to our sense of safety when the body is a constant source of never-ending pain?
The Trauma of Endometriosis
Experts define trauma as the experience of being left alone with one’s pain. Endometriosis isn’t different. Having to constantly explain one’s pain to medical doctors, families, and friends and still not being believed is an isolating and traumatizing experience. For some, this experience of being gaslit gets stored in the body and pushes the nervous system into a hypervigilant state (Fight, Flight, Freeze).
This experience of trauma can bring up various responses, anger being one of them. The anger can be at the world, the state, the body, the systems, other people, or the pain. It becomes our protective mechanism in response to the powerlessness that one feels while coping with endometriosis.
The Way Forward
In treating endometriosis, it becomes necessary to consider its impact on mental health and provide psychosocial support to people with endometriosis and their families. Unlike the conventional medical belief that solely focuses on the physiological aspects, a multidisciplinary approach integrating the mind and the body is necessary.
A trauma-informed psychotherapist specialized in treating endometriosis, and chronic pain can be helpful. A therapist trained in chronic pain management understands endometriosis, related diagnoses, and its trauma. This understanding is an integral part of the healing process. Seeing the light at the end of the tunnel is complicated and sometimes impossible with pain. Verbalizing the pain, having the hardships validated, acknowledged, and believed can be an empowering experience. Just as people seek medical help for their physical symptoms, seeking help for mental health struggles is an integral part of the endometriosis journey. If therapy is hard to access, support groups for endometriosis can be a step forward. You should know that you are not alone in your experience, and you can have support. The supports that you get can be a lifeline to your mental health.
Author: Anindita Kundu, Trauma Psychotherapist.
How has endometriosis impacted your mental health? Have you considered working with a mental health specialist to help you?

Questions to Ask Your Physical Therapist When You have Endometriosis
Author: Dr. Rebecca Patton, PT, DPT
Table of contents
- Endometriosis Care Process with iCareBetter
- 1. Are you familiar with the disease process and current treatment standards for endometriosis?
- 2. Do they consider the whole body when treating your symptoms?
- 3. Do they practice trauma-informed care specifically related to healthcare trauma?
- 4. How much time will you have for a session?
“I feel like you’re the first physical therapist who understands endo.” It’s a statement I wish I didn’t hear as often as I do. Unfortunately, there has not been a resource specifically made to evaluate pelvic physical therapists’ knowledge about endometriosis before iCareBetter.
Education for physical therapists regarding endometriosis needs more advanced continuing education courses. But it doesn’t typically happen until after completing a doctoral program. For perspective, I self-taught for several years before seeking specific classes related to endometriosis care. Therefore, it wasn’t until years after specializing in pelvic pain treatment that I realized the inefficiency of care for those with endometriosis. We can do better, but we have a long way to go.
Communicating with a pelvic physical therapist before seeking treatment can allow you to ask important questions to ensure you’re finding a provider that is a good fit for you. For achieving this goal, take advantage of time-saving strategies such as a phone consultation before committing to a therapist. Here are a few questions you may want to ask during that phone consultation or the first visit with a pelvic physical therapist for your endometriosis issues.
Endometriosis Care Process with iCareBetter
1- Find an expert based on keyword/ specialty or state
2- choose your doctor from the list
3- Get the contact info
4- First call and consultation.
5- Get info regarding costs and care process
6- Receive care
Top endometriosis physical therapists
Endometriosis Physical Therapy
1. Are you familiar with the disease process and current treatment standards for endometriosis?
It is helpful when your treating therapist is up to date on current treatment standards, as with any diagnosis. Unfortunately, there is no specific physical therapy protocol for treating patients with endometriosis. However, physical therapists should understand who will be involved in your healthcare team and have a multidisciplinary approach (1). I aim to establish what provider, either GYN or expert surgeon, will be a point of contact on that first visit.
2. Do they consider the whole body when treating your symptoms?
Endometriosis is known as a pelvic disease, but we know it is much more than that. Your physical therapist needs to tap into their education to evaluate and treat the whole body. The secondary effect of endo is often an upregulated nervous system. On the initial visit, it is typical that your physical therapist will look at movement patterns from your neck to your feet. Internal pelvic floor assessments are common but certainly do not need to happen on the first visit. Pelvic floor function is only one component in a much larger picture of your overall function. Your individual goals and comfort will dictate how much treatment involves pelvic floor treatment.
Advanced Treatments and education
Treatment involving the abdominal wall fascia, diaphragm, and viscera (organs) require additional advanced coursework compared to treating the pelvic floor. Therefore, you can ask them if they have taken additional coursework to treat the abdomen to get an idea of their experience. There is not one single treatment philosophy for the abdomen, but some courses focus on continuing education in this area. The most common that I am familiar with are The Barral Institute (2), Ramona Horton MPT, DPT (3), and Institute of Physical Art (4). Other courses involve manual nerve techniques such as Lumbar and Sacral Nerve Manual Assessment through the Herman and Wallace Pelvic Rehab Institute (5). These are just a few of the many available resources your physical therapist may use to learn more after graduate school. Some pelvic physical therapists create their treatment tanks to teach one another these skillsets.
Treatment strategies that help regulate an upregulated nervous system may be part of your care. These strategies can look like gentle hands-on treatment, questions to help you process how you relate to your body, and creating mindfulness along with movement. The connection of how our nervous system interprets information from our body is complex. A physical therapist can be a valuable resource to help you better understand the pain response and the nervous system.
3. Do they practice trauma-informed care specifically related to healthcare trauma?
Trauma-informed care in physical therapy does not substitute mental health treatment. A trauma-informed approach concerning physical therapy means understanding the entirety of the patient’s experience and the effects of that experience. Medical trauma can have a lasting response on an individual’s well-being (6). We know that those with endo, on average, have a delayed diagnosis. This delay can lead to a complicated relationship with the medical providers. Many patients with endo are seeking out pelvic PT after years of seeing various specialists. These experiences with the medical system can create barriers to a patient feeling comfortable with a new provider.
For this reason, a trauma-informed approach to treatment is essential. Awareness of how these experiences may have impacted their patient is a critical portion of providing affirming care. You can ask your physical therapist about some processes that they use to create a safe environment. These processes should include consent before any treatment or touching, checking in with your emotions and body reaction during manual therapy, and providing adequate time to provide education throughout the session.
4. How much time will you have for a session?
Asking this question can ensure you have an idea of what to expect when going into your appointment. There is no magic number of minutes that will create a perfect appointment. However, the nature of endo being more complex means I prefer more time to establish a care plan. There are multiple factors to consider during the first evaluation. These factors include sexual health, daily function, bowel and bladder health, and personal goals. Having realistic expectations for each session is helpful to decrease additional medical trauma and find a therapist that fits your needs.
Patient care and human interaction are complex, and sometimes it takes time to establish a level of comfort with your PT. Every session of PT may not equal a breakthrough in pain. Retraining the nervous system takes time, especially when the body has been protecting itself due to chronic pain.
Ultimately, endo care is ideally a multidisciplinary approach. Your physical therapist can work closely with your gynecologist and other healthcare team members to find the best individual plan for you.
If you have more questions about pelvic physical therapy, reach out for more information.
Would you mind sharing with us what pleasant or unpleasant experiences you have had with your PT?
References:
1. Agarwal SK, Foster WG, Groessl EJ. Rethinking endometriosis care: applying the chronic care model via a multidisciplinary program for the care of women with endometriosis. Int J Womens Health. 2019;11:405-410. Published 2019 Jul 23. doi:10.2147/IJWH.S207373
2. Jean-Pierre Barral, DO, MRO(F), RPT. The Barral Institute. Accessed September 1st, 2021. https://www.barralinstitute.com/
3. Ramona Horton, MPT, DPT. Herman and Wallace Pelvic Rehabilitation Institute. Accessed August 27th, 2021. https://hermanwallace.com/faculty/ramona-horton
4. Institute of Physical Art. 2015-2021. Accessed August 19th, 2021. https://instituteofphysicalart.com/
5. Nari Clemmons PT, PRPC. Herman and Wallace Pelvic Rehabilitation Institute. Accessed August 20th, 2021. https://hermanwallace.com/faculty/nari-clemons6. Michelle Flaum Hall and Scott E. Hall. When Treatment Becomes Trauma: Defining, Preventing, and Transforming Medical Trauma. American Counseling Association. March 24th, 2013. Accessed August 19th, 2021. https://www.counseling.org/knowledge-center/vistas/by-year2/vistas-2013/docs/default-source/vistas/when-treatment-becomes-trauma-defining-preventing-

A Multidisciplinary Team for Endometriosis is Key to Positive Outcomes
Table of contents
- Why Your Endometriosis Treatment Plan Should be Multidisciplinary
- What is Endometriosis?
- What is a Multidisciplinary Team Approach in Medicine?
- Benefits of a Multidisciplinary Treatment (MDT) Team for Endometriosis
- Who comprises an Endometriosis Multidisciplinary Team?
- Psychiatrist/Psychologist:
- Building Your Multidisciplinary Team for Endometriosis
Why Your Endometriosis Treatment Plan Should be Multidisciplinary
Endometriosis (endo) is a chronic and progressive disorder characterized by the growth of endometriosis tissue outside the uterus. This disorder often affects various organs in the body and results in pain and other issues. In addition to the intense physical and often debilitating symptoms of the disease, it can also take a toll on mental and spiritual health. Therefore, a multidisciplinary team (MDT) approach to endometriosis pain, surgery, and disease management leads to the best outcomes for patients. Keep reading to learn how.
What is Endometriosis?
Pronounced (en-doe-me-tree-O-sis), endometriosis is a chronic inflammatory disorder in which a type of tissue that is similar to the endometrial tissue that normally grows inside the uterus, grows outside this organ. Sometimes, the endometriosis tissue appears on the outer side of the uterus. These lesions can also grow on the ovaries, fallopian tubes, bladder wall, and on the outside of other organs within the pelvic cavity and other regions of the body.
Endometriosis is often a very painful and debilitating disease. During menstruation, these endometriosis growths shed blood into the body which is not able to be released. This causes an increase in pressure throughout the pelvic and sometimes abdominal region. Endo often involves other organs such as the bowels, ovaries, fallopian tubes, vagina, and cervix. In rare cases, it may affect other organs, such as the bladder, lungs, diaphragm, or kidneys. If you would like to learn more information about endometriosis, read our article, “Endometriosis 101: Covering the Basics”.
What is a Multidisciplinary Team Approach in Medicine?
Multidisciplinary care is when multiple members of the healthcare team come together to collaborate to provide optimal care for a patient. When it comes to endometriosis treatment, it’s important to involve various disciplines across the healthcare spectrum to achieve the best possible outcomes for patients.
Benefits of a Multidisciplinary Treatment (MDT) Team for Endometriosis
Draw in endo experts across different care areas to enhance the patient’s prospects and outcomes. Physicians benefit from this approach as they are able to provide a better framework for decision-making on a collaborative level and implementation. These aspects are particularly important when dealing with complex endometriosis cases. When several endo experts work together in unison, the benefits include cross-discipline learning, research, and review.
There is a type of disease, called deep infiltrating endometriosis (DIE). Alarmingly, about 20 percent of endo patients have this type. With DIE, the lesions can penetrate 5 mm deep into the organs affected by the disorder. A multidisciplinary treatment plan is the best approach for better outcomes and improved quality of life for the patient. The resection of DIE lesions requires a surgeon with expertise in endometriosis and a multidisciplinary approach coordinated by the endo specialist.
In fact, in 2019, the Society for Women’s Health Research assembled a team of clinicians, researchers, and patients to deliberate on the barriers in the commonly accepted forms of endometriosis treatment and management. The team underscored the importance of comprehensive and interdisciplinary approaches to disease and pain management for proper treatment and diagnosis.
Who comprises an Endometriosis Multidisciplinary Team?
The following are some of the endometriosis experts that come together and help treat patients holistically:
Endometriosis Surgeon (Gynecologist):
If you have endometriosis, a regular obstetrics-gynecological surgeon is not going to suffice. It’s important to have an endometriosis specialist, who is an OB surgeon with experience in the treatment of this pelvic disease. An endometriosis laparoscopy is often needed to diagnose and treat the disease. It’s important to choose a surgeon familiar with endo to ensure all lesions are removed. Learn more about endometriosis specialists and how to find a vetted physician in our article here.
Colorectal Surgeon (Bowel Surgeon):
If the endometriosis affects the bowel, surgical excision may be necessary to remove the lesions. Surgical treatment, such as full-thickness disc excision or a bowel resection should only be performed by an experienced colorectal surgeon. This physician will participate in the care from the diagnostic workup to surgical treatment and follow-up care.
Urologist (Genitourinary Tract Doctor):
A urologist treats disorders of the urethra, kidneys, urinary bladder, and adrenal glands. Having an experienced urologist as part of your multidisciplinary team can help aid in the treatment of ureter and bladder lesions as well as minimize kidney or bladder complications.
Radiologist Experienced in Endometriosis:
Endometriosis may have several presentations, which can make diagnostic testing challenging. Because endometriosis lesions can present in other areas of the body away from the reproductive organs, it’s important that the radiologist on your team is familiar with the pelvic nerve anatomy and how to detect signs of neural endometriosis.
Physical Therapist/Pelvic Floor Therapist:
Physical therapy can be very important in the treatment of endometriosis. While some patients may require physical therapy to help them adapt to pain and stay mobile, others may need highly specific pelvic floor therapy. A pelvic floor physical therapist can work with the patient to help reduce adhesions and scar tissue which can limit pelvic floor extensibility. These exercises are important to help reduce pain sometimes associated with intercourse or the insertion of a tampon.
Pain Management Doctor:
Endometriosis pain is often the primary complaint and most debilitating symptom of this disease. In fact, it’s not uncommon for the pain associated with endo to become so intense that a person is no longer able to function in daily life. For this reason, a pain management doctor should be a part of the team to improve functioning and overall quality of life.
Psychiatrist/Psychologist:
Anxiety and depression are two of the biggest mental health disorders that often accompany endometriosis. Furthermore, the pain and sometimes infertility that come with this disorder can further aggravate these negative emotions. Therefore, a holistic MDT for endometriosis will include a psychiatrist or psychologist, possibly one who specializes in pain management.
Nutritionist:
Nutrition plays a key role in the processes and regulation of your digestive and immune systems. A proper endometriosis diet can help to reduce the chronic inflammation that keeps the endometriosis lesions growing and spreading. A nutritionist with experience in treating endo patients is key for successful outcomes.
Pathologist:
There are different stages and types of endometriosis. Endometriosis with architectural atypia is one type that may be a precursor of ovarian cancer. Therefore, it’s important that a pathologist carefully examines the lesions to discover if they could be indicative of endometriosis-associated ovarian cancer.
Building Your Multidisciplinary Team for Endometriosis
Who’s got your back? If you have or suspect you might have endometriosis, this is a very important question to ask yourself. iCareBetter is a digital platform that connects endo patients to vetted endometriosis experts across a variety of disciplines. If you have endo, we want to hear from you. Do you already have an MDT for endo? If so, who are the members of your personal team?
