Colon Chronicles: Delving into Bowel Endometriosis
In our recent blog, we highlighted the significance of addressing bowel endometriosis, a condition prone to misdiagnosis. Whether individuals have struggled with lifelong bowel issues or are suddenly facing disruptions, determining what’s considered normal can be perplexing. The “normal” range spans anywhere from three times a day to as infrequent as three times per week. In many sources, the focus is typically limited to frequency and to some degree consistency; however, there’s an overall scarcity of information on what defines normalcy.
ICYMI: Understanding Bowel Endometriosis
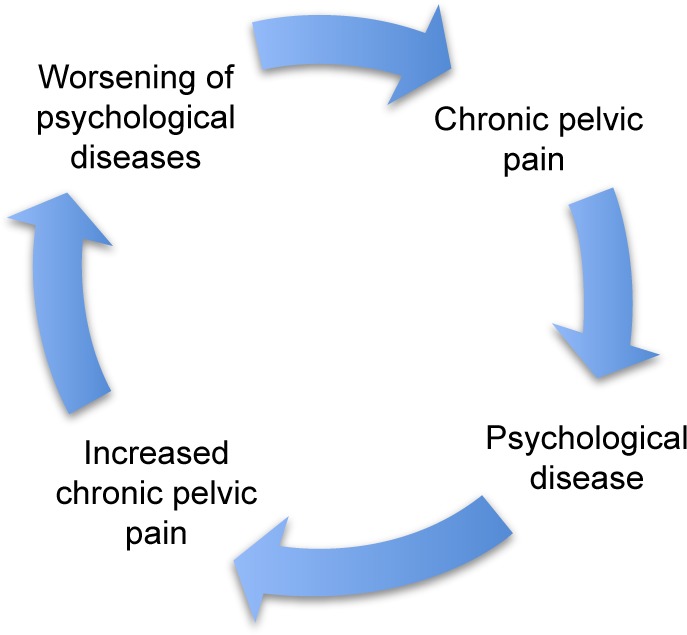
This ambiguity is particularly challenging for those with endometriosis, where gastrointestinal symptoms vary widely, making it tough to discern what’s amiss. About 90% of endometriosis cases involve some form of gastrointestinal symptoms, often leading to an IBS (irritable bowel syndrome) diagnosis, which essentially offers a label for persistent symptoms without an identifiable cause. The usual next step in diagnostics is often a colonoscopy, a key tool for identifying or ruling out certain diseases. This article explores the nuances of bowel endometriosis, with a primary focus on the role and precision of colonoscopy in diagnosing this condition.
Bowel endometriosis is considered to be deep infiltrating endometriosis and can lead to a variety of symptoms which we discussed in the previous blog, but is often concerning if not diagnosed timely and may risk more complex surgeries including resection if the disease is not properly addressed.
Related Reading: How to Get an Endometriosis Diagnosis
The Role of Colonoscopy – Is it helpful?
A colonoscopy is a diagnostic procedure commonly used to examine the inner lining of the large intestine (colon and rectum). It involves the use of a long, flexible tube called a colonoscope, which has a small camera attached to its end. This tool allows physicians to visualize the interior of the colon to identify any abnormal conditions or changes.
In the context of bowel endometriosis, a colonoscopy can potentially detect signs of endometrial tissue growth within the bowel. However, its effectiveness and accuracy in diagnosing this condition have been subjects of ongoing research and debate. Aside from its ability to detect endometriosis, there is also consideration of the provider performing the procedure and their level of knowledge of endometriosis.
The use of colonoscopy in diagnosing bowel endometriosis has been a topic of considerable discussion among medical professionals. Given the invasive nature of the procedure and the often non-specific symptoms of bowel endometriosis, the role and necessity of colonoscopy in its diagnostic process have been questioned.
However, several case studies and research findings suggest that colonoscopy can indeed play a crucial role in identifying bowel endometriosis. In particular, it has been found to be effective in detecting endometriosis growth in the bowel, with certain colonoscopic findings such as eccentric wall thickening, polypoid lesions, and surface nodularities often being associated with endometriosis.
Evaluating the Accuracy of Colonoscopy for Diagnosing Bowel Endometriosis
While the potential of colonoscopy in detecting bowel endometriosis has been recognized, its accuracy in doing so has been the subject of extensive research. A number of studies have sought to evaluate the sensitivity, specificity, and predictive values of colonoscopy in diagnosing this condition.
One such study was conducted by Milone M et al., who performed a prospective observational study that included women diagnosed with deep pelvic endometriosis. The study aimed to evaluate the accuracy of colonoscopy in predicting intestinal involvement in deep pelvic endometriosis.
The results of the study suggested that colonoscopy did have the potential to detect bowel endometriosis, with a number of cases accurately diagnosed through the procedure. However, the overall sensitivity, specificity, and predictive values of colonoscopy were found to be variable, indicating room for improvement in its diagnostic accuracy.
In another study conducted by Marco Milone and his team, the researchers also found that while colonoscopy could indeed identify bowel endometriosis, its accuracy was not optimal. The study elucidated that the presence of colonoscopic findings of intestinal endometriosis in deep pelvic endometriosis was quite low, indicating that routine colonoscopy may not be justified for all women with deep pelvic endometriosis.
A Case Study: Bowel Endometriosis and Colonoscopy
To illustrate the potential role of colonoscopy in diagnosing bowel endometriosis, let’s consider a case study involving a 45-year-old woman who presented with abdominal pain in her left lower quadrant. This woman underwent a colonoscopy, which revealed a submucosal tumor-like lesion in her sigmoid colon.
Upon further examination using magnifying endoscopy, the lesion was found to contain sparsely distributed round pits – a finding that was suggestive of endometrial glands and stroma (the histological definition of endometriosis). This discovery led to a biopsy of the lesion, the results of which confirmed the presence of intestinal endometriosis.
This case study serves to highlight how colonoscopy, when combined with other diagnostic methods like magnifying endoscopy and biopsy, can aid in the detection and diagnosis of bowel endometriosis.
The Future of Bowel Endometriosis Diagnosis
While the role and accuracy of colonoscopy in diagnosing bowel endometriosis have been explored, research in this area is ongoing. The development and refinement of diagnostic methods are crucial for improving the detection and treatment of bowel endometriosis.
In parallel with the innovations in medical technology, new diagnostic methods such as magnifying chromoendoscopy, target biopsy, and virtual colonoscopy are being explored and studied for their potential to improve the accuracy of bowel endometriosis diagnosis. These advancements, coupled with a deeper understanding of the condition, may pave the way for more accurate and less invasive diagnostic options in the future.
Bowel endometriosis is a complex condition that can significantly impact the quality of life of those affected. While colonoscopy can play a role in its diagnosis, its effectiveness and accuracy are subject to continuous research and improvement. Exploring new diagnostic methods and refining existing ones are crucial steps toward enhancing the detection and treatment of this condition. As we continue to learn more about bowel endometriosis and its nuances, we can hope for more efficient and accurate diagnostic tools in the future.
Related Reading:
- Endo-Fighting Microbiome Optimization: Research-based Tips
- Endometriosis and the Microbiome: Insights and Emerging Research
References:
- Walter SA, Kjellström L, Nyhlin H, Talley NJ, Agréus L. Assessment of normal bowel habits in the general adult population: the Popcol study. Scand J Gastroenterol. 2010;45(5):556-566. doi:10.3109/00365520903551332
- Habib, N., Centini, G., Lazzeri, L., Amoruso, N., El Khoury, L., Zupi, E., & Afors, K. (2020). Bowel Endometriosis: Current Perspectives on Diagnosis and Treatment. Int J Womens Health, 12, 35-47. https://doi.org/10.2147/IJWH.S190326
- Milone, M., Mollo, A., Musella, M., Maietta, P., Sosa Fernandez, L. M., Shatalova, O., Conforti, A., Barone, G., De Placido, G., & Milone, F. (2015). Role of colonoscopy in the diagnostic work-up of bowel endometriosis. World J Gastroenterol, 21(16), 4997-5001. https://doi.org/10.3748/wjg.v21.i16.4997
- Tomiguchi, J., Miyamoto, H., Ozono, K., Gushima, R., Shono, T., Naoe, H., Tanaka, M., Baba, H., Katabuchi, H., & Sasaki, Y. (2017). Preoperative Diagnosis of Intestinal Endometriosis by Magnifying Colonoscopy and Target Biopsy. Case Rep Gastroenterol, 11(2), 494-499. https://doi.org/10.1159/000475751

Through the Looking Glass: Reflecting on 2023
Embarking on the journey of self-reflection is not just a personal endeavor; for us at iCareBetter, it’s a collective celebration of progress, community, and collaboration. As we bid farewell to 2023, a year marked by challenges and triumphs, it’s time to take a look into the past year and reflect on all that has been accomplished. Join us as we navigate through the areas of growth, community involvement, projects, and meaningful collaborations that shaped our year. In this special blog post, we’re excited to share the insights gained from our podcast endeavors and offer a sneak peek into the thrilling developments that await us in 2024. Let’s rewind, recap, and anticipate the exciting narrative that continues to unfold in the ever-evolving story of iCareBetter.
About iCareBetter
iCareBetter is an innovative platform dedicated to helping patients with endometriosis and chronic pelvic pain find compassionate and skilled experts. All experts on iCareBetter have shown knowledge and expertise in the treatment of endometriosis and chronic pelvic pain.
Vision
Our vision is to reduce the symptom-to-effective treatment of endometriosis to less than a year. Studies show that patients with endometriosis spend an average of 7.5 years to have an official diagnosis. Moreover, even after the diagnosis, patients will have to spend several years with multiple failed treatment attempts. After the long delays in diagnosis and treatment, they might be lucky enough to receive effective treatment from an expert.
Mission
Our mission is to improve access to high-quality specialized care for those with endometriosis. iCareBetter wants to combat the issue of patients living in confusion, pain, and isolation. To that end, we hope to connect as many patients to the right experts as early as possible. And we hope that this will ensure timely diagnosis and effective treatment.
To read more about why iCareBetter was built and the inspiration behind it, check out our blog here and listen to episode 1 of the podcast here, where Saeid and Jandra give you a behind the scenes look into what inspired them.
What happened in 2023?
In 2023, iCareBetter grew in many ways, including new avenues to provide education along with collaboration from the community. Here are some of the highlights!
- We started a podcast! iCareBetter: Endometriosis Unplugged is hosted by Jandra Mueller, DPT, MS a pelvic floor physical therapist and endometriosis patient. The podcast is available on Spotify, Apple Podcasts, and Youtube.
- We had 19 weekly episodes in season one
- Listeners joined from all over the world, reaching 22 countries
- We brought on a team to help with new content on social media creating a more visually appealing platform, community engagement, and followers.
- We now have 211 providers on our website available and ready to help those suffering from endometriosis and we are continuing to grow!
- Our blog content is now consistent with twice weekly posts bringing you updates on all things endometriosis.
What To Expect in 2024
While 2023 was a big year for iCareBetter, we hope to continue the growth and expand our providers across the globe. Our hope is to increase our collaboration with medical specialists, researchers, and advocates. There are some exciting things to come in 2024 including a new season of iCareBetter: Endometriosis Unplugged as well as some other projects that will be announced in 2024.
We hope you have found our resources helpful either for yourself or a loved one, and hope you continue to share the love and spread the word about Endometriosis. All of us here at iCareBetter wish you a safe and happy new year.

Cheers to 2024!
Do you or a loved one have Endometriosis? Here are some blogs that may help you get started on your journey.
- Endometriosis Signs and Symptoms: Everything You Need to Know
- Endometriosis Facts & Myths: Dispelling the Misconceptions
Endometriosis and the Microbiome: Insights and Emerging Research
Endometriosis is a multifaceted, heterogenous, inflammatory condition that impacts 10%-15% of women (XX) in their reproductive years, most commonly associated with chronic pelvic pain and infertility.
Over the years, numerous theories have been proposed to explain its pathogenesis, but none have conclusively clarified its origins. Recently, however, researchers have begun investigating the complex interplay between endometriosis and the human microbiome. This article aims to provide an in-depth exploration of the current research into the relationship between endometriosis and the microbiome, with a particular focus on gut health, inflammation, and pathogenesis.
Understanding Endometriosis
Endometriosis is marked by the growth of endometrial-like tissue found outside of the uterine cavity. This tissue is commonly found implanted over visceral and peritoneal surfaces within the abdominopelvic cavity, but can extend to the connective tissue and organs throughout the body. The condition can lead to severe dysmenorrhea, pelvic pain, and subfertility among a number of other symptoms and manifestations, significantly impairing a person’s quality of life.4
Read more: What causes endometriosis?
The Human Microbiome and Its Role in Health and Disease
The human microbiome comprises microorganisms that colonize our bodies and play crucial roles in nutrient metabolism and various physiological functions. The composition and balance of these microbial communities can significantly influence our health. For instance, the gut microbiota synthesizes vitamins B12 and K, maintains intestinal mucosal integrity, promotes angiogenesis and epithelial repair, and modulates immune functions.5
Disruptions in gut microbiota composition, a state known as dysbiosis, can contribute to the development and progression of numerous diseases, including inflammatory bowel diseases, arthritis, psoriasis, neuropsychiatric diseases, and even malignancies.4 Given that endometriosis is a chronic inflammatory disease potentially triggered by altered immune functions and increased angiogenesis, there is a growing interest in investigating the role of microbiota dysbiosis in the pathogenesis and pathophysiology of endometriosis.1,4
The Microbiome-Endometriosis Connection: An Emerging Field of Research
Recent studies have commenced exploring whether microbiome composition is altered in women with endometriosis. For instance, one study identified significant differences in the microbial community structure between those with and without endometriosis.1,5 This study found that the abundance of Acinetobacter, Pseudomonas, Streptococcus, and Enhydrobacter significantly increased, while the abundance of Propionibacterium, Actinomyces, and Rothia significantly decreased in the endometriosis group.5
Another study focused on the microbiota of extracellular vesicles in the peritoneal fluid.4,5 These vesicles, small structures made of bilayered lipid membranes released by cells, carry proteins, nucleic acids, and lipids, and play a key role in immune function, inflammatory reactions, and disease development. Like other cells, bacteria can release extracellular vesicles that modulate host-cell immune responses and other health conditions. The study found significant differences in the microbial community of these vesicles between women with and without endometriosis.5
Highlighting the complex relationship between the microbiome and endometriosis, several studies have shown an increased bacterial colonization of menstrual blood and endometrial tissue in women with endometriosis compared to control subjects.5 A study on rhesus monkeys demonstrated that altered composition of the intestinal microflora and intestinal inflammation are associated with endometriosis. While we know animal comparison is not exactly like humans, the reproductive tract of rhesus monkeys closely resembles humans in both the form and function.7
Read more: Endo-Fighting Microbiome Optimization: Research-based Tips
Microbiome and the Inflammatory Response in Endometriosis
Endometriosis is known to trigger an inflammatory response within the body, characterized by increased production of pro-inflammatory cytokines, autoantibodies, growth factors, oxidative stress, and alterations in T-cell and natural killer cell reactivity.1 This dysregulated immune response potentially creates an immunosuppressive environment that enables the growth of these endometriosis lesions.1
Recent studies suggest that gut microbiome-derived extracellular vesicles could play a critical role in this process.5 These vesicles, ranging from 20 to 400 nm in diameter, can traverse the intestinal barrier, enter the systemic circulation, and potentially influence the peritoneal environment. They may carry a cargo of proteins, nucleic acids, and lipids that can influence immune function, inflammatory responses, and the development of diseases like endometriosis.
One study demonstrated that extracellular vesicles from women with endometriosis carry unique cargo that can influence inflammation, angiogenesis, and proliferation.5 Another study identified specific proteins in the exosomes of peritoneal fluid samples from patients with endometriosis, suggesting a role of exosomes in the diagnosis and treatment of endometriosis.5
The Gut Microbiome and Estrogen Levels
The gut microbiome is a significant regulator of estrogen levels, influencing estrogen metabolism and hence potentially affecting estrogen-dependent diseases like endometriosis.3 In postmenopausal women, fecal microbiota richness and levels of fecal Clostridia taxa have been associated with systemic estrogen levels. Therefore, gut dysbiosis leading to abnormal circulating levels of estrogen could potentially play a role in the development of endometriosis or the associated symptoms.3
The Microbiome as a Diagnostic and Therapeutic Target
The alterations in microbiota composition associated with endometriosis may provide valuable diagnostic markers for the disease. For instance, one study has proposed a microbiota-based model that can distinguish infertile patients with and without endometriosis.1 Another study has found that specific bacterial species are enriched in the endometrium and peritoneal fluid of patients with endometriosis.2
On the therapeutic front, the modulation of gut microbiota through dietary interventions, prebiotics, probiotics, or fecal microbiota transplantation could potentially represent a novel treatment approach for endometriosis.4 However, more research is needed to explore the potential of these strategies and to understand the precise mechanisms through which the microbiota influences endometriosis development and progression.
Read More: Integrative Therapies for Endometriosis
Conclusion
The complex relationship between the microbiome and endometriosis is still in its early stages of investigation. Recent studies indicate that alterations in microbiota composition may be associated with endometriosis. These insights not only enhance our understanding of endometriosis pathogenesis but also open up new possibilities for the diagnosis and treatment of this prevalent condition.
As our understanding of the microbiome continues to grow, so does the potential for novel, integrative health strategies that target this complex ecosystem. Further research is required to confirm the observed associations and to elucidate the mechanisms underlying the microbiome-endometriosis connection. Such research holds the promise of ushering in a new era in our approach to endometriosis, one that acknowledges the intricate interplay between our bodies and the microbes that inhabit them.
While there are limitations in the current usefulness of this research, we do know that the immune system is involved with regulating the disease. An important question remains: are the microbiota changes seen in those with endo the chicken or the egg?
References:
- Leonardi, M., Hicks, C., El-Assaad, F., El-Omar, E., & Condous, G. (2020). Endometriosis and the microbiome: a systematic review. BJOG, 127(2), 239-249. https://doi.org/10.1111/1471-0528.15916
- Oishi, S., Mekaru, K., Tanaka, S. E., Arai, W., Ashikawa, K., Sakuraba, Y., Nishioka, M., Nakamura, R., Miyagi, M., Akamine, K., & Aoki, Y. (2022). Microbiome analysis in women with endometriosis: Does a microbiome exist in peritoneal fluid and ovarian cystic fluid? Reprod Med Biol, 21(1), e12441. https://doi.org/10.1002/rmb2.12441
- Svensson, A., Brunkwall, L., Roth, B., Orho-Melander, M., & Ohlsson, B. (2021). Associations Between Endometriosis and Gut Microbiota. Reprod Sci, 28(8), 2367-2377. https://doi.org/10.1007/s43032-021-00506-5
- Jiang, I., Yong, P. J., Allaire, C., & Bedaiwy, M. A. (2021). Intricate Connections between the Microbiota and Endometriosis. Int J Mol Sci, 22(11). https://doi.org/10.3390/ijms22115644
- Lee, S. R., Lee, J. C., Kim, S. H., Oh, Y. S., Chae, H. D., Seo, H., Kang, C. S., & Shin, T. S. (2021). Altered Composition of Microbiota in Women with Ovarian Endometrioma: Microbiome Analyses of Extracellular Vesicles in the Peritoneal Fluid. Int J Mol Sci, 22(9). https://doi.org/10.3390/ijms22094608
- Wei, W., Zhang, X., Tang, H., Zeng, L., & Wu, R. (2020). Microbiota composition and distribution along the female reproductive tract of women with endometriosis. Ann Clin Microbiol Antimicrob, 19(1), 15. https://doi.org/10.1186/s12941-020-00356-0
- Burns, K. A., Pearson, A. M., Slack, J. L., Por, E. D., Scribner, A. N., Eti, N. A., & Burney, R. O. (2021). Endometriosis in the Mouse: Challenges and Progress Toward a ‘Best Fit’ Murine Model. Front Physiol, 12, 806574. https://doi.org/10.3389/fphys.2021.806574