

Endometriosis Myths & Facts: Dispelling the Misconceptions
Table of contents
- Debunking the Myths About Endometriosis & Exploring the Facts
- Overview of Endometriosis
- Why is it Difficult to Diagnose Endometriosis?
- Myth #1: Severe Period Pain is Normal
- Myth #2: A Hysterectomy Cures Endometriosis
- Myth #3: Endometriosis Only Affects the Pelvic Area
- Myth #4: Endometriosis Symptoms are Simply a “Heavy Period”
- Myth #5: Douching Causes Endometriosis
- Myth #6: Having an Abortion Can Cause Endometriosis
- Myth #7: You’re Too Young to Have Endometriosis
- Myth #8: Endometriosis Can Be Prevented
- Myth #9: Endometriosis is Always Painful
- Myth #10: Pregnancy is a Cure for Endometriosis
- Myth #11: Menopause Cures Endometriosis
- Myth #12: Hormonal Therapy Cures Endometriosis
- Myth #13: Endometriosis is Cancer
- Myth #14: Tubal Endometriosis Always Causes Infertility
- Myth #15: Endometriosis Symptoms Are the Results of Emotional Distress (It Is All in Your Head)
- We Want Your Input
Debunking the Myths About Endometriosis & Exploring the Facts
One in ten women worldwide is affected by endometriosis, also known as “endo,” for short. While this number is an estimate, the actual figures may be higher. Not only is the person with this inflammatory disorder affected, so are the family members and people around her due to the often debilitating effects of this disease. Endometriosis facts are important because it is complex and often misunderstood even though it’s a common disorder. Because of this, there are many myths and misconceptions regarding endometriosis prognosis, treatment, causes, symptoms, diagnosis, complications, etc.
Focusing on the disease itself often ignores the vicious cycles of stress, fatigue, pain, doctor visits, flare-ups, and loss of productivity experienced by the patient. These factors can lead to a decreased quality of life. Worse is that endometriosis facts come behind outdated treatment options, myths, and misconceptions about this disorder. It takes an average of eight to ten years for a patient to be diagnosed with endometriosis. One of the biggest problems with the misconceptions about endo is that they can prevent women from seeking treatment. Keep reading as we review endometriosis facts and debunk the myths.
Overview of Endometriosis
Endometriosis is a pelvic disorder characterized by endometriosis tissue similar but not the same as the tissue inside the uterus, growing elsewhere. Typically, the growth occurs outside the uterus, ovaries, fallopian tubes, cervix, the surface of the bladder, bowel, and distant organs.
Endometriosis growths can cause pain, scarring, and sometimes infertility. Pain from endometriosis is usually the result of menstrual bleeding from the tissues. Unlike the endometrium inside your uterus, blood that comes from endo tissue outside this organ has no means of escaping the body. This blood causes increased pressure and inflammation, which can result in pain that’s often debilitating. If you would like to learn more information about endometriosis, please read our introduction article, “Endometriosis 101: Covering the Basics.”
Why is it Difficult to Diagnose Endometriosis?
Studies show that it can take an average of seven years or more for a woman to get an endometriosis diagnosis. Why is this? Endometriosis signs and symptoms are often similar to other conditions, such as irritable bowel syndrome or pelvic inflammatory disease (PID). Therefore, it’s often mistaken for another illness. Furthermore, the myths and misconceptions we discuss below also prevent a lot of women from seeking help. For this reason, it’s crucial to get the endometriosis facts clear. Keep reading as we debunk the myths and state the facts.
Myth #1: Severe Period Pain is Normal
Nineteenth-century doctors were often perplexed by “women’s problems.” As a result, women were often discounted as being unstable mentally. While the attitudes and thoughts have improved since, some of those old beliefs persist, including those regarding period pain.
Many patients with endometriosis hear that their severe period pain is “normal.” Pain and cramping are normal during menstruation. However, the pain should not be so intense that it interferes with functioning or impacts the quality of life. If your period pain is so severe that you cannot carry out daily activities, you should seek an endometriosis expert.
Myth #2: A Hysterectomy Cures Endometriosis
Endometriosis growths are tissues “similar” to those inside of the uterus. It is not the same tissue. Simply removing the uterus and/or ovaries without excising any endometriotic implants growing outside the uterus will not cure it.
Myth #3: Endometriosis Only Affects the Pelvic Area
Locations within the pelvis, such as the surface of the uterus, bladder, or fallopian tubes, are the most common locations where endometriosis growths occur. However, endo can occur elsewhere in the body. In some cases, endometriosis growths have been present in distant organs, such as the lungs.
Myth #4: Endometriosis Symptoms are Simply a “Heavy Period”
Bleeding during menstruation can be heavy at times. However, it should not exceed the saturation of a pad or tampon in one hour. If you experience that degree of bleeding, you should bring this up with your healthcare provider. The fact is that many women with endometriosis experience abnormally heavy flow due to the excess tissue.
Myth #5: Douching Causes Endometriosis
No scientific evidence links douching with the development of endometriosis.
Myth #6: Having an Abortion Can Cause Endometriosis
No scientific evidence demonstrates that having an abortion causes endometriosis. Those who claim otherwise might be confusing endometritis and endometriosis.
Myth #7: You’re Too Young to Have Endometriosis
A common misconception is that endometriosis is rare or doesn’t occur in young women and teenagers. As a result, many doctors do not consider an endometriosis diagnosis in young women with typical symptoms. Endometriosis facts demonstrate that teenagers and women in their early 20s can have the disorder. Most people with endometriosis state they experienced endo symptoms during adolescence.
Myth #8: Endometriosis Can Be Prevented
It’s not clearly understood what causes endometriosis. Therefore, there are no proven ways to prevent this inflammatory condition. Anything else is purely speculation at this point.
Myth #9: Endometriosis is Always Painful
Not all women with endometriosis experience pain. Studies show that some women with advanced stages of endometriosis do not experience pain as a symptom.
Myth #10: Pregnancy is a Cure for Endometriosis
This misconception about endometriosis is slowly beginning to fade. However, not quickly enough! Pregnancy fluctuates hormones in the female body, which can temporarily suppress some symptoms of endometriosis. However, these symptoms usually recur for most patients following the pregnancy. Therefore, it’s not a cure.
Myth #11: Menopause Cures Endometriosis
Endometriosis symptoms often occur during menstruation, but many women experience them long after periods stop. Following menopause, the body still produces small amounts of hormones, and the endometriosis tissue still responds to them, thus causing pain. For many women, the symptoms of endometriosis may improve after menopause, but that does not mean it’s a cure. Depending on the case, it might be necessary to remove endometriosis implants or adhesions even after menopause.
Myth #12: Hormonal Therapy Cures Endometriosis
Doctors have been treating endometriosis for years using hormonal therapy drugs. However, these medications do not have long-term effects on the disease itself. Hormones can help relieve the symptoms temporarily and even shrink the growths, but they do not cure endometriosis.
Myth #13: Endometriosis is Cancer
Endometriosis growths are not cancerous. To date, there is little evidence that shows endometriosis directly causes cancer. However, some types of cancers are more common in women who have endometriosis. Endometrial cancer is also known as uterine cancer. Many studies have examined the relationship between the two, and one showed that merely 0.7 percent of patients with endometriosis had endometrial cancer at the 10-year follow-up. Therefore, endometriosis does not equal cancer, but it may increase the risk of cancer.
Myth #14: Tubal Endometriosis Always Causes Infertility
Tubal endometriosis is not very common, and it does not always cause infertility. Does endometriosis cause infertility? It can be in many cases, but the mechanisms of infertility in endometriosis remain multifactorial. Can you get pregnant with endometriosis? It is possible, and many women do – especially with proper treatment early on.
Myth #15: Endometriosis Symptoms Are the Results of Emotional Distress (It Is All in Your Head)
Yes. People have heard many times that emotional distress could be the cause of their endometriosis and pain. This statement is false. The fact is, endometriosis is a highly complex disorder with many underpinnings. Those with endometriosis often experience emotional distress as an impact of the symptoms such as pain and infertility. But emotional distress it’s not the cause of endometriosis symptoms.
Endometriosis quick facts:
1- There is no blood test available for the diagnosis of endometriosis.
Mehedintu C, J Med Life, 2014
2- The diagnosis of endometriosis starts by taking a good history from patients, and performing a detailed physical exam including pelvic exam. In some cases, a doctor might ask for MRI and Ultrasound to have a more thorough picture. But the ultimate diagnosis is only possible with laparoscopic /robotic surgery and taking a biopsy for histopathology. There is no blood test that can tell if you have endometriosis.
3- Studies show that those with endometriosis have an increased risk of developing depression and anxiety disorders.
Chen LC, et al, J Affect Disord, 2016
4- Pelvic pain due to endo occurs a day part of an inflammatory cycle which can affect the pelvic organs and functions such as sitting, sex, bowel movements and even urination. Pelvic floor physical therapy can help with restoring balance to the pelvic floor muscles.
Dr. Juan Michelle Martin, Endometriosis Physical Therapist.
5- “The most common clinical signs of endometriosis are menstrual irregularities, chronic pelvic pain, dysmenorrhea (painful periods), dyspareunia (painful sex), and infertility.”
Lagana AS, et al, Int J Womens Health. 2017
We Want Your Input
Are there any endometriosis myths or misconceptions we did not list here? Let us know in the comments below!

Pelvic Congestion Syndrome- another cause of chronic pelvic pain
When talking about endometriosis and chronic pelvic pain, it is important to remember that often endometriosis is not the only pelvic pain generator. Another possible contributor to chronic pelvic pain is pelvic congestion syndrome (PCS). PCS is like having varicose veins in the pelvis. Blood pulls in the veins and can cause symptoms such as heaviness, pain with penetration, noncyclical pain, positional lower back pain, pelvic and upper thigh pain, prolonged postcoital discomfort, symptoms that worsen throughout the day and are exacerbated by activity or prolonged standing, and non-specific lower abdominal and pelvic pain (Durham & Machan, 2013; Mistry & le Roux, 2017). LIANG and Brown (2021) report that:
“Typical pelvic congestion syndrome pain is:
– Heaviness and dull aching in nature
– Located deep in the pelvis and on the left
– Exacerbated by upright position (standing or sitting) and exercise (walking, running, weightlifting)
– Worse towards the end of the day
– Worse after sexual intercourse
– Worse when bladder is full
– Chronic and insidious onset
Atypical pelvic congestion syndrome pain is:
– Constant pain not related to time of day, upright posture or physical activities
– Pain worse premenstrually and during menstrual periods
– More on the right than the left
– Acute and sudden onset
– Sharp or colicky in nature”
While the gold standard for diagnosis is contrast venogram, this procedure is usually done as part of the treatment (embolization procedure) (LIANG & Brown, 2021). LIANG and Brown (2021) report that “all non-invasive imaging like ultrasound, CT and MRI can detect pelvic varicosities” but that the key is “to alert the imaging technicians and specialist to look out for pelvic varicosities and to report them” (LIANG & Brown, 2021). A CT scan can also help diagnose other syndromes such as Nutcracker Syndrome (left renal vein compression) and May-Thurner Syndrome (left iliac vein compression) (LIANG & Brown, 2021). If you’ve had surgeries before for endometriosis and wonder why it wasn’t seen during surgery, it is because surgery “is performed with the patient in supine or Trendelenburg position, and with the use of CO2 for abdominal distention” thus meaning that the “veins are often collapsed, and pelvic varicosities can be missed”- it would take the surgeon who suspects pelvic varicosities to put the patient in “reverse Trendelenburg position and easing off CO2 distention” that “might allow the dilated veins to fill” and possibly be seen (LIANG & Brown, 2021).
Unfortunately, PCS doesn’t just go away or improve with time, therefore, treatment is usually needed for those who are symptomatic (LIANG & Brown, 2021). Because there is pooling and back flow of blood in the veins, the treatment suggested is transcatheter embolization (LIANG & Brown, 2021). Medication, hysterectomy, and other treatments have not proved as effective (LIANG & Brown, 2021). The transcatheter embolization “is performed with conscious sedation under local anaesthetic, as a day procedure” and “is one of the safest embolisation procedures” (LIANG & Brown, 2021). LIANG and Brown (2021) report that “some feel the relief of pelvic congestion syndrome symptoms soon after embolisation, while others might have to wait for the thrombophlebitis to settle before appreciating the result”- reporting that it is best to wait 4-6 weeks to better judge the effectiveness. Mistry & le Roux (2017) report that after looking at 20 studies that “the overall technical success rate was as high as 99%” and that “with a mean follow up of 15 months, 80% of the patients reported benefit from the procedure while 13% experienced little or no relief of the symptoms”.
PCS may be another piece in the puzzle of ongoing chronic pelvic pain.
References
Durham, J. D., & Machan, L. (2013, December). Pelvic congestion syndrome. In Seminars in interventional radiology (Vol. 30, No. 04, pp. 372-380). Thieme Medical Publishers. Retrieved from https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0033-1359731
LIANG, D. E., & Brown, B. (2021). Pelvic congestion syndrome: Are we missing the diagnosis?. The Medical Republic. Retrieved from https://www.sydneyfibroidclinic.com.au/app/uploads/2021/06/PCS-Medical-Republic.pdf
Mistry, P. P., & le Roux, D. A. (2017). Pelvic congestion syndrome (PCS). Practice Perspectives for Venous Disorders, 46. Retrieved from http://www.vascularsociety.co.za/wp-content/uploads/2019/02/VASSA-venous-guidelines-Practice-perspectives-for-venous-disorders-2017.pdf#page=46

A Multidisciplinary Team for Endometriosis is Key to Positive Outcomes
Table of contents
- Why Your Endometriosis Treatment Plan Should be Multidisciplinary
- What is Endometriosis?
- What is a Multidisciplinary Team Approach in Medicine?
- Benefits of a Multidisciplinary Treatment (MDT) Team for Endometriosis
- Who comprises an Endometriosis Multidisciplinary Team?
- Psychiatrist/Psychologist:
- Building Your Multidisciplinary Team for Endometriosis
Why Your Endometriosis Treatment Plan Should be Multidisciplinary
Endometriosis (endo) is a chronic and progressive disorder characterized by the growth of endometriosis tissue outside the uterus. This disorder often affects various organs in the body and results in pain and other issues. In addition to the intense physical and often debilitating symptoms of the disease, it can also take a toll on mental and spiritual health. Therefore, a multidisciplinary team (MDT) approach to endometriosis pain, surgery, and disease management leads to the best outcomes for patients. Keep reading to learn how.
What is Endometriosis?
Pronounced (en-doe-me-tree-O-sis), endometriosis is a chronic inflammatory disorder in which a type of tissue that is similar to the endometrial tissue that normally grows inside the uterus, grows outside this organ. Sometimes, the endometriosis tissue appears on the outer side of the uterus. These lesions can also grow on the ovaries, fallopian tubes, bladder wall, and on the outside of other organs within the pelvic cavity and other regions of the body.
Endometriosis is often a very painful and debilitating disease. During menstruation, these endometriosis growths shed blood into the body which is not able to be released. This causes an increase in pressure throughout the pelvic and sometimes abdominal region. Endo often involves other organs such as the bowels, ovaries, fallopian tubes, vagina, and cervix. In rare cases, it may affect other organs, such as the bladder, lungs, diaphragm, or kidneys. If you would like to learn more information about endometriosis, read our article, “Endometriosis 101: Covering the Basics”.
What is a Multidisciplinary Team Approach in Medicine?
Multidisciplinary care is when multiple members of the healthcare team come together to collaborate to provide optimal care for a patient. When it comes to endometriosis treatment, it’s important to involve various disciplines across the healthcare spectrum to achieve the best possible outcomes for patients.
Benefits of a Multidisciplinary Treatment (MDT) Team for Endometriosis
Draw in endo experts across different care areas to enhance the patient’s prospects and outcomes. Physicians benefit from this approach as they are able to provide a better framework for decision-making on a collaborative level and implementation. These aspects are particularly important when dealing with complex endometriosis cases. When several endo experts work together in unison, the benefits include cross-discipline learning, research, and review.
There is a type of disease, called deep infiltrating endometriosis (DIE). Alarmingly, about 20 percent of endo patients have this type. With DIE, the lesions can penetrate 5 mm deep into the organs affected by the disorder. A multidisciplinary treatment plan is the best approach for better outcomes and improved quality of life for the patient. The resection of DIE lesions requires a surgeon with expertise in endometriosis and a multidisciplinary approach coordinated by the endo specialist.
In fact, in 2019, the Society for Women’s Health Research assembled a team of clinicians, researchers, and patients to deliberate on the barriers in the commonly accepted forms of endometriosis treatment and management. The team underscored the importance of comprehensive and interdisciplinary approaches to disease and pain management for proper treatment and diagnosis.
Who comprises an Endometriosis Multidisciplinary Team?
The following are some of the endometriosis experts that come together and help treat patients holistically:
Endometriosis Surgeon (Gynecologist):
If you have endometriosis, a regular obstetrics-gynecological surgeon is not going to suffice. It’s important to have an endometriosis specialist, who is an OB surgeon with experience in the treatment of this pelvic disease. An endometriosis laparoscopy is often needed to diagnose and treat the disease. It’s important to choose a surgeon familiar with endo to ensure all lesions are removed. Learn more about endometriosis specialists and how to find a vetted physician in our article here.
Colorectal Surgeon (Bowel Surgeon):
If the endometriosis affects the bowel, surgical excision may be necessary to remove the lesions. Surgical treatment, such as full-thickness disc excision or a bowel resection should only be performed by an experienced colorectal surgeon. This physician will participate in the care from the diagnostic workup to surgical treatment and follow-up care.
Urologist (Genitourinary Tract Doctor):
A urologist treats disorders of the urethra, kidneys, urinary bladder, and adrenal glands. Having an experienced urologist as part of your multidisciplinary team can help aid in the treatment of ureter and bladder lesions as well as minimize kidney or bladder complications.
Radiologist Experienced in Endometriosis:
Endometriosis may have several presentations, which can make diagnostic testing challenging. Because endometriosis lesions can present in other areas of the body away from the reproductive organs, it’s important that the radiologist on your team is familiar with the pelvic nerve anatomy and how to detect signs of neural endometriosis.
Physical Therapist/Pelvic Floor Therapist:
Physical therapy can be very important in the treatment of endometriosis. While some patients may require physical therapy to help them adapt to pain and stay mobile, others may need highly specific pelvic floor therapy. A pelvic floor physical therapist can work with the patient to help reduce adhesions and scar tissue which can limit pelvic floor extensibility. These exercises are important to help reduce pain sometimes associated with intercourse or the insertion of a tampon.
Pain Management Doctor:
Endometriosis pain is often the primary complaint and most debilitating symptom of this disease. In fact, it’s not uncommon for the pain associated with endo to become so intense that a person is no longer able to function in daily life. For this reason, a pain management doctor should be a part of the team to improve functioning and overall quality of life.
Psychiatrist/Psychologist:
Anxiety and depression are two of the biggest mental health disorders that often accompany endometriosis. Furthermore, the pain and sometimes infertility that come with this disorder can further aggravate these negative emotions. Therefore, a holistic MDT for endometriosis will include a psychiatrist or psychologist, possibly one who specializes in pain management.
Nutritionist:
Nutrition plays a key role in the processes and regulation of your digestive and immune systems. A proper endometriosis diet can help to reduce the chronic inflammation that keeps the endometriosis lesions growing and spreading. A nutritionist with experience in treating endo patients is key for successful outcomes.
Pathologist:
There are different stages and types of endometriosis. Endometriosis with architectural atypia is one type that may be a precursor of ovarian cancer. Therefore, it’s important that a pathologist carefully examines the lesions to discover if they could be indicative of endometriosis-associated ovarian cancer.
Building Your Multidisciplinary Team for Endometriosis
Who’s got your back? If you have or suspect you might have endometriosis, this is a very important question to ask yourself. iCareBetter is a digital platform that connects endo patients to vetted endometriosis experts across a variety of disciplines. If you have endo, we want to hear from you. Do you already have an MDT for endo? If so, who are the members of your personal team?

How Do I Know If I Have Endometriosis? Endometriosis Signs
Table of contents
Learn Endometriosis Signs & Symptoms & What to Tell Your Doctor
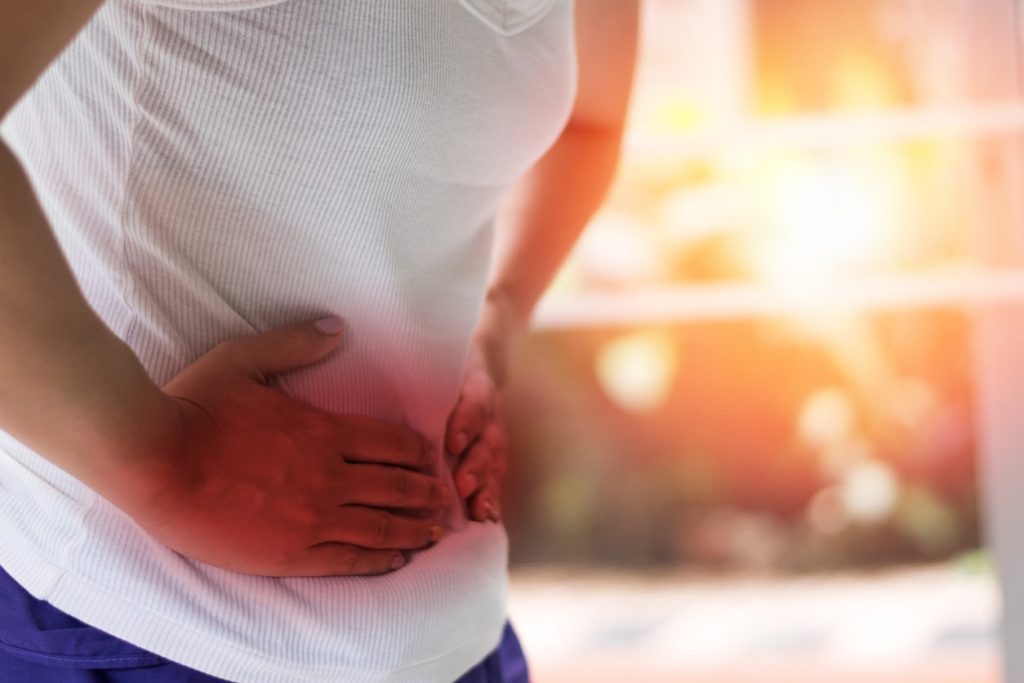
Pelvic pain is common for most women during their period. However, for some – this time of the month comes with excruciating pain due to the medical condition – endometriosis (also known as endo for short). Believe it or not, endometriosis signs extend beyond just the debilitating pain, although, that’s the hallmark symptom of this inflammatory disorder.
If you think you might have endometriosis, it’s important to have a solid foundation of information before you see your doctor for a possible endo diagnosis. Keep reading to learn what endometriosis is and what are the most common signs and symptoms of this condition.
What Is Endometriosis?
Pronounced (en-doe-me-tree-O-sis), endometriosis is a chronic inflammatory disorder of the pelvis where tissue similar to that normally grows inside your uterus, grows elsewhere instead, usually on the outside of it. The endometriosis tissue can block fallopian tubes, cover your ovaries, and even line the organs of your pelvis.
Endometriosis can cause intense pain and fatigue, which makes it a disabling inflammatory condition for many women. Pain from endometriosis can be so intense that sometimes even medication cannot touch it. Other organs commonly involved include the fallopian tubes, bowels, cervix, ovaries, vagina, and pelvic tissue. Rarely, endo may also affect distant organs. Learn more about the disorder in our previous article, “Endometriosis 101: Covering the Basics”.
What Are Endometriosis Signs and Symptoms?
Sadly, endometriosis is an inflammatory disorder that often goes undiagnosed for years because the hallmark symptoms are things that some women take for granted as “normal”: heavy bleeding and pain during periods. If you think you might have endometriosis, it’s important that you know what to look for and when you should notify a doctor. The following are seven common signs of endometriosis:
Dysmenorrhea (Painful Periods):
Intense pelvic or abdominal pain is one of the most common symptoms of endometriosis. Endometriosis pain is often described as a sharp or stabbing sensation. During menstruation, women with endo may experience very painful periods because the endometrial tissue swells and bleeds every month, just like the uterine lining would. However, because this process is occurring outside the uterus, blood is not easily shed, and this pressure can cause extreme cramping that is much more intense than typical period cramps. Period pain should not disrupt your daily life, so if it does, you need to let your doctor know or find a qualified endo specialist.
Menorrhagia (Heavy Menstrual Bleeding):
While many women bleed heavily during their period, endometriosis can cause significant blood loss. How do you know if your amount of bleeding is excessive? Watch for these signs:
- Passing large clots
- Period goes on longer than a week
- Bleeding through a pad or tampon in an hour
- Too fatigued to carry out daily activities
If you have these symptoms, you may have menorrhagia and should contact a gynecologist. Menorrhagia is sometimes caused by endometriosis, and it can cause anemia and severe fatigue.
Dyspareunia (Pain During or After Intercourse):
When endometriosis is the cause of painful intercourse, the woman may not experience the pain upon entry, only upon deep penetration. There can be physical and psychological causes of this condition, and endometriosis may be the culprit, as tissue builds up on the other side of the lower uterus or vagina – and sexual intercourse can stretch the tissue. You should talk to an experienced physician if you have pain during or after intercourse.
Chronic Pelvic Pain:
While the inflammatory condition usually involves pain during menstruation, endometriosis pain can occur at any time of the month. Endometriosis causes an increase in pressure due to the excessive tissue in the pelvic cavity. This can cause a chronic pain condition that might be felt exclusively in the pelvis or manifest as abdominal or back pain.
Ovarian Cysts:
There is a type of endometriosis that causes endometriomas (also known as chocolate cysts) to grow on your ovaries. These cysts are non-cancerous but may become large and painful. Also, women who have these may also have other endometrial growths in the abdominal or pelvic areas.
Infertility:
Up to about half of women who have problems with fertility also have endometriosis. Furthermore, up to 50 percent of women who have endometriosis are unable to get or stay pregnant. The relationship between these conditions isn’t always clear as many factors can impact fertility. However, in the event that the endometriosis tissue blocks the reproductive organs, there is a clear connection. Treating the condition can increase your odds of having a baby. If these fertility issues are affecting you, contact an endometriosis specialist.
Bowel/Bladder Problems:
Bathroom visits may be problematic if you have endometriosis lesions growing near your bladder or bowels. And if you are experiencing difficulty with urination or bowel movements or bleeding in the bowel – these may be signs of endometriosis. Also, if you have painful urination, blood in your stool, nausea, or hyper urgency to urinate – you should tell your medical provider immediately.
When to Call Your Healthcare Provider
Share with your healthcare provider any of the following endometriosis signs and symptoms:
- Pain. Pain is the most common sign of endometriosis, and it can be present:
- During or after sex
- With bowel movements
- When urinating during your period
- As chronic abdominal, lower back, or intestinal pain
- Similar to menstrual cramps that get worse gradually
- Bleeding or spotting between periods
- Difficulty getting pregnant or infertility
- Digestive issues or stomach problems such as diarrhea, constipation, bloating, or nausea—especially during your periods

Genes associated with endometriosis
It’s an exciting title: “Genetic cause of endometriosis discovered, pointing to new drug therapy” (Haridy, 2021). But it is misleading. When you look further, it reveals it is referencing a study (Tapmeier et al., 2020) that identified “a novel genetic variant that is associated with severe cases of endometriosis” (Haridy, 2021). The article further states that “NPSR1 mutations have never before been linked with endometriosis” but “they have, however, been associated with inflammatory diseases including arthritis, inflammatory bowel disease and asthma” (Haridy, 2021). This gene was noted in endometriosis patients in a 2016 study that identified several genes associated with endometriosis (Houshdaran et al., 2016). The article also notes “not every woman with endometriosis was found to have this particular NPSR1 variant, affirming the heterogenous nature of the condition” and that the gene has a “potential role in endometriosis” that “points to the development of anti-inflammatory therapeutics targeting this mechanism” (Haridy, 2021).
We know there is a genetic component to endometriosis; however, a single gene has not been identified as the cause. This study notes that this particular gene is associated with stage III/IV endometriosis and with other inflammatory conditions. The research is identifying new potential drug targets to help with symptoms.
Genetics account for about 50% of the risk for endometriosis with the other 50% “likely owing to environmental factors” (Montgomery et al., 2020). “As with other complex diseases, genetic variants in the DNA sequence increasing endometriosis risk all have small effects, unlike most single-gene disorders” and “it is the combinations of these variants adding together that contribute to higher risks for individual women” (Montgomery et al., 2020). The science of epigenetics should also be considered.
Epigenetics is “the study of biological mechanisms that will switch genes on and off” (What Is Epigenetics, 2019). Epigenetics can be influenced by almost everything: “what you eat, where you live, who you interact with, when you sleep, how you exercise, even aging – all of these can eventually cause chemical modifications around the genes that will turn those genes on or off over time” (What Is Epigenetics, 2019). Epigenetics involved with endometriosis might include “DNA methylation and histone modification, and, other non-classic mechanisms: miRNAs and lncRNA” (Chen et al., 2020). “Increased estrogen activity and progesterone resistance are the main hormonal substrate of this disease and are associated with inflammatory response and debilitating symptoms, including pain and infertility….The regulation of receptor expression by epigenetics maybe a critical factor for endometriosis” (Chen et al., 2020).
In short, endometriosis is pretty complicated and we still have much to learn.
References
Chen, H., Malentacchi, F., Fambrini, M., Harrath, A. H., Huang, H., & Petraglia, F. (2020). Epigenetics of estrogen and progesterone receptors in endometriosis. Reproductive Sciences, 1-8. Retrieved from https://link.springer.com/article/10.1007/s43032-020-00226-2
Haridy, R. (2021). Genetic cause of endometriosis discovered, pointing to new drug therapy. Retrieved from https://newatlas.com/science/genetic-cause-endometriosis-inflammation-new-drug-therapy/
Houshdaran, S., Nezhat, C. R., Vo, K. C., Zelenko, Z., Irwin, J. C., & Giudice, L. C. (2016). Aberrant endometrial DNA methylome and associated gene expression in women with endometriosis. Biology of reproduction, 95(5), 93-1. Retrieved from https://doi.org/10.1095/biolreprod.116.140434
Montgomery, G. W., Mortlock, S., & Giudice, L. C. (2020). Should genetics now be considered the pre-eminent etiologic factor in endometriosis?. Journal of minimally invasive gynecology, 27(2), 280-286. Retrieved from https://doi.org/10.1016/j.jmig.2019.10.020
Tapmeier, T. T., Rahmioglu, N., Lin, J., Obendorf, M., de Leo, B., Montgomery, G., … & Zondervan, K. T. (2020). Neuropeptide S Receptor 1 is a Novel Non-Hormonal Treatment Target in Endometriosis. Reproductive Sciences, 27(SUPPL 1), 130A-130A. Retrieved from https://stm.sciencemag.org/content/13/608/eabd6469
What Is Epigenetics. (2019). A Super Brief and Basic Explanation of Epigenetics for Total Beginners. Retrieved from https://www.whatisepigenetics.com/what-is-epigenetics/

Endometriosis Doctor For Diagnosis, Treatment, & Surgery
Why Is It Crucial for Your OB-GYN to Be an Endometriosis Doctor?
When it comes to the treatment and management of endometriosis pain and/or other symptoms, all doctors are not the same. In fact, if you have or suspect you might have endometriosis, you may be left disappointed with the answers (or lack thereof) you receive from a general obstetrician/gynecologist (OB-GYN).
It can be a bit tricky to find an endometriosis doctor who is highly skilled and follows the best endometriosis treatment and management practices for this disorder. If you want to learn more about endometriosis, read this article that gives an introduction to the condition, signs and symptoms, causes, complications, and treatments.
With so many myths about endometriosis (endo), it’s important to separate facts from fiction. Arm yourself with research and a solid foundation of knowledge to help you simplify the process and get in touch with a trusted endometriosis doctor. Keep reading to find out why it’s so important to use an endo expert, red flags that your doctor/surgeon is not the right fit, and how to find an endometriosis doctor near you.
Join the endometriosis forum or Instagram page and discover endometriosis stories and discussions.
Understanding Endometriosis: An Overview
Endometriosis, a perplexing and often debilitating condition, affects a significant number of people assigned females at birth, primarily during their reproductive years. It occurs when endometrial-like tissue, which typically lines the uterus, implants and grows outside the uterine cavity. These lesions can have debilitating effects on the body, mediated by estrogen, they produce inflammation and can create structural changes due to scarring and adhesions, ultimately contributing to chronic pelvic pain and, in some cases, infertility.
Endometriosis is a primary contributor to infertility among women, as the tissue implants can interfere with ovarian function or obstruct the fallopian tubes. In severe cases, the tissue may even spread beyond the pelvic region, affecting other organs. While the exact cause remains elusive, researchers have proposed theories involving retrograde menstruation, genetic predispositions, and immune system dysfunction.
Symptoms: Recognizing the Signs
The symptoms of endometriosis can vary widely among individuals, ranging from mild discomfort to severe, debilitating pain. Common manifestations include:
- Pelvic or lower back pain during menstrual periods
- Painful intercourse
- Abnormally heavy or prolonged menstrual bleeding
- Infertility
- Fatigue
- Painful urination or bowel movements during menstruation
- Digestive issues like diarrhea, constipation, or nausea
If you experience persistent or worsening symptoms, it is crucial to seek medical attention promptly.
The Diagnostic Journey: Unveiling Endometriosis
Diagnosing endometriosis can be challenging, as the symptoms may mimic those of other conditions. Your healthcare provider will typically begin by reviewing your medical history and performing a physical and pelvic examination. However, a definitive diagnosis often requires a laparoscopic procedure.
During a laparoscopy, a thin, lighted instrument called a laparoscope is inserted through a small incision in the abdominal wall, allowing the surgeon to visualize the pelvic area and identify any endometrial tissue implants. In some cases, a biopsy may be performed to confirm the diagnosis.
Additional tests, such as ultrasounds, CT scans, or MRI scans, may be ordered to assess the extent and location of the endometrial lesions, particularly if deep infiltrating endometriosis (DIE) is suspected, where the tissue grows into surrounding organs like the bowel or bladder.
The Pivotal Role of Endometriosis Specialists
![]()
![]()
While general gynecologists can provide initial evaluations and basic treatment options, endometriosis specialists are uniquely qualified to manage this complex condition effectively. The right specialist will have extensive knowledge of this disorder and the additional surgical training and skills it takes to effectively treat endo and related conditions. These specialists, typically obstetrician-gynecologists (OB/GYNs) or reproductive endocrinologists, possess extensive knowledge and surgical expertise in treating endometriosis and related conditions.
Endometriosis specialists are trained to utilize advanced surgical techniques, such as laparoscopic or robotically assisted procedures, to meticulously remove endometrial lesions and scar tissue. They have access to state-of-the-art equipment and a comprehensive understanding of various treatment modalities, including hormonal therapies, pain management strategies, and complementary approaches.
Moreover, these specialists often collaborate with a multidisciplinary team of professionals, including colorectal surgeons, urologists, pain management specialists, and mental health professionals, to provide holistic care tailored to each patient’s unique needs. The openness to complementary treatments and a thorough understanding of various treatments are some other advantages of choosing an endometriosis doctor and not just a regular OBGYN.
Red Flags About a Potential Endometriosis Doctor Expert
It’s important that you pick an expert who knows what they’re doing to support you. Unfortunately, there are a lot of myths surrounding surgical best practices when it comes to endo treatment. What’s even worse is that some of these options could result in infertility or other issues, and not even address the underlying endometriosis condition.
The following are red flags that could indicate the doctor you are speaking with is not a trusted endometriosis specialist:
- If the doctor views hysterectomy as a definitive treatment. Caution any doctor who says removing your uterus/ovaries will cure you. While this may be the correct course for some patients, it’s not a cure-all solution as endo lesions can affect other body parts and endo tissue could continue to grow.
- If the doctor says endo symptoms will go away with menopause. In medically, naturally, and surgically-induced menopause, there are women who have endometriosis afterward.
- If the doctor says mild stages of endometriosis won’t cause infertility. This is just false. “Mild” or “minimal” stages of endo can still produce significant symptoms, including those that impact fertility.
- If the doctor says that negative tests rule out an endo diagnosis. Tests such as labs, ultrasound, or magnetic resonance imaging (MRI) can help with the diagnosis and staging of endometriosis, but they cannot rule it out. Technology has advanced, and transvaginal ultrasound can help in assessing and staging endometriosis; however, it cannot rule out the diagnosis. The same is true for MRIs and laboratory studies.
- Hormone therapy will cure endometriosis. Studies show that hormonal medications may help temporarily reduce endometrial lesions (possibly) and manage symptoms, but they do not cure the disease.
- If the doctor suggests that recurring endometriosis cannot be treated.
- If the doctor tells you that you are too young to have endometriosis. This belief is completely false. In fact, there are adolescents who had chronic pelvic pain that were diagnosed with deep infiltrating endometriosis (DIE).
- If the doctor suggests it’s only irritating bowel syndrome (IBS). Many symptoms of endometriosis and IBS overlap. As such, this is often a misdiagnosis given to people who, in fact, are suffering from endometriosis. Please notice that this doesn’t mean that the patient doesn’t also have IBS in conjunction with endo.
Treatment Options: A Comprehensive Approach
The treatment approach for endometriosis is highly individualized, taking into account factors such as symptom severity, fertility goals, and overall health status. Endometriosis specialists typically employ a combination of medical and surgical interventions to alleviate symptoms and address underlying issues.
Medical Management
For individuals not actively seeking pregnancy, hormonal therapies are often the first line of treatment. These medications aim to suppress ovarian function and manage symptoms of endometriosis. Common options include:
- Combined hormonal contraceptives (birth control pills, patches, rings, or injections)
- Gonadotropin-releasing hormone (GnRH) agonists or antagonists
- Progestin therapy (levonorgestrel-releasing intrauterine devices, contraceptive implants, or oral progestins)
- Aromatase inhibitors (in combination with other hormonal therapies)
While these medications can effectively manage symptoms for some, they are not curative and may have side effects such as hot flashes, vaginal dryness, or bone loss. Endometriosis specialists can guide patients through the potential risks and benefits of each option.
In cases of severe pain or discomfort, nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen may be recommended for pain relief, either alone or in conjunction with hormonal therapies.
Surgical Intervention
The gold standard for diagnosing endometriosis is laparoscopic surgery with histological diagnosis. Meaning, that during surgery, you are diagnosed, and when the lesions are removed, they are sent to a pathologist who will confirm the diagnosis. Ideally, a proper excision surgery should be performed at the same time as the diagnosis. Endometriosis specialists are trained in various surgical techniques, ranging from minimally invasive laparoscopic procedures to more extensive open surgeries, depending on the severity of the endometriosis and the training they’ve had.
Laparoscopic surgery, often referred to as “conservative surgery,” aims to preserve the uterus and ovaries while removing endometriosis lesions, adhesions, and scar tissue. This approach can improve fertility outcomes and alleviate pain, but endometriosis may recur over time. However, in some cases, a hysterectomy may be performed laparoscopically in addition to endometriosis excision if there are other concerns, such as adenomyosis, and fertility is not desired.
Complementary Therapies
In addition to traditional medical and surgical treatments, endometriosis specialists may recommend complementary therapies to manage pain and improve overall well-being. These may include:
- Physical therapy to relax pelvic floor muscles and alleviate pelvic pain
- Acupuncture, which has shown promising results in reducing endometriosis-related pain
- Dietary modifications and supplements (e.g., omega-3 fatty acids, magnesium)
- Mind-body practices like meditation, yoga, or cognitive-behavioral therapy to reduce stress and improve coping mechanisms
It is essential to discuss any complementary therapies with your healthcare provider to ensure they are safe and appropriate for your individual situation.
Seeking Fertility Treatment
For women with endometriosis who are struggling to conceive, endometriosis doctors can collaborate with reproductive endocrinologists to develop a comprehensive fertility treatment plan. Options may include ovulation-inducing medications, intrauterine insemination (IUI), or in vitro fertilization (IVF).
IVF, in particular, has shown promising results for women with endometriosis, as it bypasses potential obstacles caused by the condition, such as blocked fallopian tubes or impaired ovarian function. Endometriosis doctors can provide guidance on the most appropriate fertility treatment based on the individual’s age, severity of endometriosis, and overall health status and recommend a tailored treatment plan as to when would be the most ideal time for these types of treatments.
Finding the Right Endometriosis Doctor
Choosing the right endometriosis doctor is crucial for effective diagnosis and treatment. When seeking a specialist, consider the following factors:
- Experience: Look for specialists who have extensive experience in treating endometriosis and related conditions, particularly in performing advanced surgical techniques.
- Qualifications: Endometriosis specialists should be board-certified OB/GYNs or reproductive endocrinologists with specialized training in endometriosis management and specialized in treating fertility problems.
- Communication and rapport: A good specialist should actively listen to your concerns, explain treatment options in clear and understandable terms, and foster a collaborative relationship.
- Multidisciplinary approach: Specialists who work closely with other healthcare professionals, such as colorectal surgeons, pain management specialists, and mental health professionals, can provide more comprehensive care.
- Accessibility: Consider the specialist’s location, availability, and affiliation with reputable medical centers or hospitals that regularly treat endometriosis.
Additionally, seeking recommendations from trusted sources, such as support groups, online forums, or your primary care physician, can aid in finding a qualified endometriosis specialist in your area.
Endometriosis Support and Resources
Living with endometriosis can be physically and emotionally challenging. Seeking support from others who understand the condition’s impact can be invaluable. Consider joining a local or online support group where you can share experiences, receive practical advice, and find a sense of community.
Additionally, numerous reputable organizations and websites offer educational resources, up-to-date research findings, and support services for individuals with endometriosis. These resources can empower you with knowledge and provide guidance throughout your journey.
Conclusion: Embracing Hope and Empowerment
Endometriosis is a complex condition that requires specialized care and a multifaceted approach to treatment. By partnering with an experienced endometriosis specialist, you can navigate the diagnostic process, explore various treatment options, and develop a personalized plan tailored to your specific needs and goals.
While the journey may be challenging, embracing a proactive and informed approach can empower you to take control of your health and improve your overall quality of life. With the right support and guidance, it is possible to manage endometriosis effectively and find relief from its debilitating symptoms.
Remember, you are not alone in this journey. By seeking out knowledgeable healthcare professionals, connecting with supportive communities, and advocating for your well-being, you can overcome the obstacles posed by endometriosis and reclaim your vitality.
REFERENCES :
https://icarebetter.com/endometriosis-specialist-for-diagnosis-treatment-surgery/
https://nyulangone.org/care-services/endometriosis-center
https://www.endofound.org/preparing-to-see-a-doctor
https://www.mayoclinic.org/diseases-conditions/endometriosis/diagnosis-treatment/drc-20354661
https://www.uwmedicine.org/conditions-symptoms/reproductive-sex-organs/endometriosis

What a Pain! Vaginismus, Vulvodynia, and More
Endometriosis can have a cascade effect on the muscles, fascia, and nerves of the pelvis. Myofascial pain is involved in up to 94% of chronic pelvic pain and can occur “independently or in conjunction with disorders such as vaginismus, dysmenorrhea, and endometriosis and is frequently a causative factor in sexual pain or dyspareunia” (Ross et al., 2021). Vaginismus, vulvodynia, and pudendal neuralgia are a few of things that can contribute to chronic pelvic pain.
Vaginismus is the “recurrent involuntary tightening of muscles around the vagina” (spasms) whenever penetration is attempted- such as “the use of tampons, penetrative intercourse, cervical examinations, and other activities” (Haire, 2021). Phenomena such as endometriosis, recurrent bladder infections (or painful bladder syndrome), yeast infections, hormonal changes (such as decreased lubrication with menopause) are a few of the things that might trigger it (HealthDirect, 2019). Therapies might include pelvic floor physiotherapy, local anesthetics (such as lidocaine), muscle relaxants (such as medications/creams or even botulinum toxin injections), and/or anxiolytic medication (Lahaie et al., 2010).
Vulvodynia is “chronic discomfort in the vulvar region” (Reed, 2006). The pain has been “described as ‘burning,’ but it may be irritating, sharp, prickly, or, occasionally, pruritic, and it can be mild to severe” (Reed, 2006) (pruritic meaning itching). Reed (2006) also reports that “the pain can begin suddenly when provoked, and it tends to dissipate gradually; women with vulvodynia often report hours to days of discomfort after intercourse or a pelvic examination.” The pain with vulvodynia can be exacerbated by prolonged sitting, tight clothes, riding a bike, use of tampons, or intercourse (Reed, 2006). Vulvodynia might be contributed to by “injury to, or irritation of, the nerves that transmit pain from the vulva to the spinal cord, an increase in the number and sensitivity of pain-sensing nerve fibers in the vulva, elevated levels of inflammatory substances in the vulva, an abnormal response of different types of vulvar cells to environmental factors such as infection or trauma, genetic susceptibility to chronic vestibular inflammation, chronic widespread pain and/or inability to combat infection, or pelvic floor muscle weakness, spasm or instability” (National Vulvodynia Association, n.d.). The National Vulvodynia Association has good information on treatment options here: https://www.nva.org/what-is-vulvodynia/treatment/.
Another entity associated with pain in the pelvic region is pudendal neuralgia. This is “a painful condition caused by inflammation, compression or entrapment of the pudendal nerve; it may be related to or be secondary to childbirth, pelvic surgery, intense cycling, sacroiliac skeletal abnormalities or age-related changes” (Perez-Lopez & Hita-Contreras, 2014). Symptoms usually present with “pelvic pain with sitting which increases throughout the day and decreases with standing or lying down, sexual dysfunction and difficulty with urination and/or defecation” (Perez-Lopez & Hita-Contreras, 2014). Treatment options might include “physiotherapy, analgesics and nerve block, surgical pudendal nerve decompression, radiofrequency and spinal cord stimulation” (Perez-Lopez & Hita-Contreras, 2014).
The pelvic floor is a busy highway of muscles, nerves, ligaments, blood vessels (see Pelvic Congestion Syndrome), and more. There is a lot that can contribute to chronic pelvic pain, and it is important to address all the factors that might be contributing to it. You can find more information here:
- https://icarebetter.com/pudendal-neuralgia-vulvodynia/
- https://icarebetter.com/pelvic-floor-dysfunction
References
Haire, G. (2021). When the Body Says No: The Experience of Vaginismus and the Validity of Female Pain. Brief Encounters. Retrieved from https://kar.kent.ac.uk/89429/1/document.pdf
HealthDirect. (2019). Vaginismus. Retrieved from https://www.healthdirect.gov.au/vaginismus
Lahaie, M. A., Boyer, S. C., Amsel, R., Khalifé, S., & Binik, Y. M. (2010). Vaginismus: a review of the literature on the classification/diagnosis, etiology and treatment. Women’s Health, 6(5), 705-719. Retrieved from https://journals.sagepub.com/doi/full/10.2217/WHE.10.46
Perez-Lopez, F. R., & Hita-Contreras, F. (2014). Management of pudendal neuralgia. Climacteric, 17(6), 654-656. Retrieved from https://doi.org/10.3109/13697137.2014.912263
National Vulvodynia Association. (n.d.). Retrieved from https://www.nva.org/
Reed, B. D. (2006). Vulvodynia: diagnosis and management. American family physician, 73(7), 1231-1238. Retrieved from https://www.aafp.org/afp/2006/0401/p1231.html
Ross, V., Detterman, C., & Hallisey, A. (2021). Myofascial Pelvic Pain: An Overlooked and Treatable Cause of Chronic Pelvic Pain. Journal of Midwifery & Women’s Health, 66(2), 148-160. Retrieved from https://doi.org/10.1111/jmwh.13224

What are the First Signs and Symptoms of Endometriosis: Everything You Need to Know
Table of contents
- What is the Endometrium?
- What is Endometriosis Pain?
- Mechanisms of Signs and Symptoms of Endometriosis :
- Painful Periods (dysmenorrhea)
- Diarrhea During Menstrual Periods
- Pain During Intercourse (Dyspareunia)
- Abdominal or Pelvic Pain After Vaginal Sex
- Painful Urination During or Between Menstrual Periods (Dysuria)
- Painful Bowel Movements During or Between Menstrual Periods (Dyschezia)
- Gastrointestinal Problems, Including Bloating, Diarrhea, Constipation, and Nausea
- Causes of Endometriosis
- Complications of Endometriosis
- Diagnosis of Endometriosis
- Treatment for Endometriosis
- Surgical Treatment Options for Endometriosis:
- Multidisciplinary Care
Sharp. Stabbing. Burning. Throbbing. Aching. All these adjectives have been used to describe endometriosis pain. Endometriosis is a condition that, for some women, can cause excruciating uterus pain. Some describe it as feeling like their insides are being pulled out of their bodies. Even worse – endometriosis pain medication doesn’t cut through or provide relief for many patients with this condition. Therefore, an endometriosis diagnosis can be very serious and life-changing news.
Our commitment to our patients runs deep, and our mission is to help patients with endometriosis pain and other complications find the skilled doctors they need.
As our first introduction to the disorder, we will give you a brief overview of the signs and symptoms of endometriosis, its causes, complications, and treatment options (or, as we like to call it – hope). First, we will give you general information on the disease and cover what endometriosis is.
What is the Endometrium?
The endometrium, also known as the endometrial lining, is the tissue that comprises the “wallpaper”, or lining of the uterus. The uterus is the pear-shaped organ that houses a growing baby. During pregnancy and menstruation, the endometrium plays vital functions.
What is Endometriosis Pain?
Endometriosis is pronounced (en-doe-me-tree-O-sis). Endometriosis is a medical condition in which tissue similar to what normally lines the inner walls of the uterus, also known as the endometrium, grows outside the uterus. It is often a very painful, even debilitating disorder. It may involve the ovaries, fallopian tubes, bowels, vagina, cervix, and the tissues that line the pelvis. In rare cases, it can also affect other organs, such as the bladder, kidneys, or lungs.
Signs and Symptoms of Endometriosis Pain
Not all women will experience the same symptoms of endometriosis or degree of intensity/severity. Some women may not experience any symptoms at all.
It is also important to keep in mind that the severity of symptoms is not a solid indicator of the progress of the disease. There are women with advanced stages of endometriosis who experience no symptoms at all and others with mild cases who endure many. Common endometriosis pain symptoms include:
- Painful periods, or dysmenorrhea
- Infertility
- Diarrhea during period
- Pain during intercourse
- Heavy or abnormal menstrual flow
- Abdominal or pelvic pain after vaginal sex
- Painful urination during or between menstrual periods
- Painful bowel movements during or between menstrual periods
- Gastrointestinal problems, including bloating, diarrhea, constipation, and/or nausea
Mechanisms of Signs and Symptoms of Endometriosis:
Painful Periods (dysmenorrhea)
Cyclic release of multiple inflammatory factors activates nerve fiber growth, leads to cell damage and fibrosis, and exacerbates pain during periods.
Infertility
The overall mechanisms can include tubal blockage, local inflammation, uterine muscle dysfunction, local hormonal alterations, and much more.
Diarrhea During Menstrual Periods
Diarrhea may result from endometriosis growing directly on the rectal muscle or endometriosis inflammatory substances. Local production of inflammatory molecules can lead to hyper-motility of the sigmoid and rectum muscles, which can manifest as cramping and diarrhea.
Pain During Intercourse (Dyspareunia)
Endometriosis implants have more nerve endings than usual (hyperinnervated) and can produce pain with pressure. The act of intercourse can apply this pressure on the upper vaginal area and uterosacral ligaments, which are common locations of endo implants. Once this pain occurs and local inflammation further causes tension in the pelvic floor, the muscles surrounding the vagina can contract, which worsens the problem.
Heavy or abnormal menstrual flow
Endometriosis can impact your bleeding by increasing stress from pain or damage to the ovaries, which can change local hormonal function.
Abdominal or Pelvic Pain After Vaginal Sex
Uterine and pelvic floor spasms are part of regular orgasms. When these areas are hypersensitive due to endometriosis, spasms lead to continued contractions and pain that lasts for a while. In addition, rectal fusion to the posterior vaginal wall will also cause more direct pain and inflammation by the vaginal area pulling on the rectal wall. Also, as you probably recognize, any event that stirs up the pelvis and causes some trauma leads to increased molecular signaling, further amplifying the problem.
Painful Urination During or Between Menstrual Periods (Dysuria)
Painful and frequent urination is a prevalent symptom of endometriosis. Endo cells and responding inflammatory cells produce inflammatory molecular signals that aggregate in the area of injury. These molecular signals affect all pelvic organs, including the bladder, leading to bladder wall spasms. Moreover, interstitial cystitis is common in endometriosis patients and can also be a factor. In the worst-case scenario, endo lesions implant inside the bladder, which can also cause cyclic bleeding from the bladder (hematuria).
Painful Bowel Movements During or Between Menstrual Periods (Dyschezia)
Endometriosis causes inflammation and fibrosis or scarring as your body attempts to heal. This inflammation and fibrosis can severely alter the anatomy in the pelvis and distort the rectal course, gluing it to the uterus, cervix, and posterior vaginal wall. This angulation can cause constipation and trouble evacuating stool, while the inflammatory signals cause the rectal muscles to hyper-contract. These mechanisms lead to painful bowel movements, which worsen during the cyclic increases in inflammatory molecules. In the worst-case scenario, the endo will grow through the rectum wall over time, causing cyclic rectal bleeding.
Gastrointestinal Problems, Including Bloating, Diarrhea, Constipation, and Nausea
Generally, intestinal symptoms of endometriosis can be direct or indirect or related to conditions like small intestinal bacterial overgrowth (SIBO). Even if there are no direct implants on the bowel, the endo inside the abdomen and pelvis can cause enough inflammation to irritate the intestine and cause symptoms. In addition, endometriosis implants directly on the bowel can worsen the symptoms.
Causes of Endometriosis
One cause of endometriosis is the direct transplantation of endometrial cells into the abdominal wall during a medical procedure, such as a cesarean section. Besides this known cause of endometriosis, other theories exist as to how it develops:
1. One theory is that during the menstrual cycle, a reverse process takes place where the tissue backs up through the fallopian tubes and into the abdominal cavity, where it attaches and grows.
2. Another theory is a genetic link. This is based on studies that show if someone has a family member with endometriosis, they are more likely to have it as well.
3. Some also suggest that the endometrial tissues travel and implant in other body parts via blood or lymphatic channels, like cancer cells spread.
4. A fourth theory suggests that all cells throughout the body have the ability to transform into endometrial cells.
Complications of Endometriosis
The following are complications of endometriosis if left untreated or in advanced stages of the disorder:
- Infertility/subfertility
- Chronic pelvic pain that can result in disability
- Anatomic disruption of involved organ systems (i.e., adhesions, ruptured cysts, renal failure)
Diagnosis of Endometriosis
The diagnosis starts with assessing signs and symptoms and then performing imaging studies such as MRI and ultrasonography. But the confirmation or exclusion of the endometriosis diagnosis is only possible with surgical biopsy and histopathology. Laparoscopy is the gold-standard surgical modality for diagnosis in all cases.
Treatment for Endometriosis
Endometriosis needs a multidisciplinary team approach for effective and holistic treatment. This team should include the following medical professionals:
- Nutritionist
- Physical therapist
- Endometriosis surgeon
- Mental health therapist
- Pain management specialist
Pain is often the biggest complaint from patients with endometriosis. Therefore, many treatment options are aimed at pain control. So first, here are some options for women to help temporarily ease the pain of endometriosis:
- Exercise
- Meditation
- Breath work
- Heating pads
- Rest and relaxation
- Prevention of constipation
These therapies may be used in combination with medical and/or surgical options to lessen the pelvic pain associated with this disorder. Furthermore, alternative therapies exist that may be used in conjunction with other interventions, and those include but are not limited to:
- Homeopathy
- Immune therapy
- Allergy management
- Nutritional approached
- Traditional Chinese medicine
*Be sure to discuss any of these treatment options with a physician before implementing them.
The Right Medical Treatment For You:
Options for medical and/or surgical treatments for endometriosis are going to depend on several factors, including:
- Desire for pregnancy
- The extent of the disease
- Type and severity of symptoms
- Patient opinions and preferences
- Overall health and medical history
- Expectations of the course of the disease
- Patients’ tolerance level for medications, therapies, and/or procedures
In some cases, management of pain might be the only treatment. In others, medical options may be considered. The following are typical non-surgical, medical treatments for endometriosis:
- “Watch and Wait” approach, where the course of the disease is monitored and treated accordingly
- Pain medication (anything from non-steroidal anti-inflammatory drugs [NSAIDs] to other over-the-counter and/or prescription analgesics)
- Hormonal therapy, such as:
- Progestins
- Oral contraceptives with both estrogen and progestin to reduce menstrual flow and block ovulation
- Danazol (a synthetic derivative of the male hormone testosterone)
- Gonadotropin-releasing hormone antagonist, which stops ovarian hormone production
Surgical Treatment Options for Endometriosis:
Despite their effectiveness in symptom control, pain medications can have significant side effects. Moreover, these medications do not stop the progression of the disease, and symptoms might return once stopped. But on the other side, surgery can lead to long-term relief and can prevent further damage to tissues. Your treatment plan should be a shared decision based on your desires, goals, and abilities.
Almost all endometriosis surgical procedures are laparoscopic or robotic. These are minimally invasive surgeries in which small tubes with lights and cameras are inserted into the abdominal wall. It allows the doctor to see the internal organs and remove endometriosis.
Excision of Endometriosis
In this technique, a surgeon cuts out much or all of the endometriosis lesions from the body. Therefore, surgeons avoid leaving any endometriosis lesions behind while preserving normal tissues. This technique is widely adopted by highly skilled endometriosis surgeons who are world leaders.
Ablation of Endometriosis
In this technique, a surgeon burns the surface of the endometriosis lesions and leaves them in the body. Most top experts highly criticize this ablation method. Ablation is most popular with surgeons who have not received enough training to do excision. As a result, these surgeons are not comfortable performing excision, and they do the ablation.
Hysterectomy
this is a surgery in which surgeons remove the uterus and sometimes ovaries. But, many surgeons consider hysterectomy an outdated and ineffective treatment for endometriosis. Almost all top endometriosis surgeons reject doing it unless there is a clear indication for hysterectomy such as adenomyosis.
Laparotomy
this surgical procedure cuts and opens the abdomen and does not use thin tubes. Therefore it is more extensive than a laparoscopy. Very few surgeons still do laparotomy because of its complications. Almost none of the top endometriosis surgeons do laparotomy for endometriosis.
Multidisciplinary Care
Along with effective surgical treatment, the patient should start working with endometriosis experts in physical therapy, mental health, nutrition, and pain management to achieve the best possible outcome.
Get in touch with Dr. Steve Vasilev
Pain with sex
A little spoken of symptom of endometriosis is pain with sex. In medical terms, it is called dyspareunia- meaning pelvic pain that occurs before, during, or after intercourse (although similar pain can also be felt with an exam or insertion of a tampon). Deep dyspareunia is “a cardinal symptom of endometriosis” (Wahl et al., 2020) with more than half of women with endometriosis experiencing it (Yong, 2017). This can play a significant role in the quality of life and relationships (Denny & Mann, 2007). The pain has been described cramping, stabbing, or stinging- among other things.
Yong (2017) proposes a classification of four types of deep dyspareunia in people with endometriosis: “type I that is directly due to endometriosis; type II that is related to a comorbid condition; type III in which genito-pelvic pain penetration disorder is primary; and type IV that is secondary to a combination of types I to III.” Fritzer and Hudelist (2017) found that “surgical excision of endometriosis is a feasible and good treatment option for pain relief and improvement of quality of sex life in symptomatic women with endometriosis.” Excision surgery for endometriosis overall shows improvement in pain with sex; however, other factors such as adenomyosis or painful bladder syndrome (interstitial cystitis) can continue to cause symptoms and should be addressed (Crispi et al., 2021). “Myofascial or nervous system mechanisms may be important for deep dyspareunia in women with endometriosis, even in those with moderate-to-severe disease (Stage III/IV)” (Orr et al., 2018). While it may feel embarrassing to bring up, it is an important aspect of your health to discuss with your provider. They might suggest pelvic floor therapy, medication, or other options to help. But it is important to address any underlying conditions.
In the meantime, some things to try:
- Have open communication with your partner about what you are feeling and your needs
- Experiment with different times of your cycle that may be less painful (such as the week after ovulation or the first couple of weeks after your period)
- Use of a lubricant
- Try different positions to find which is best for you
- Utilizing forms of intimacy that does not involve penetration
Find more here: https://icarebetter.com/pain-with-penetration/
References
Crispi Jr, C. P., Crispi, C. P., de Oliveira, B. R. S., de Nadai Filho, N., Peixoto-Filho, F. M., & Fonseca, M. D. F. (2021). Six-month follow-up of minimally invasive nerve-sparing complete excision of endometriosis: What about dyspareunia?. Plos one, 16(4), e0250046. Retrieved from https://doi.org/10.1371/journal.pone.0250046
Denny, E., & Mann, C. H. (2007). Endometriosis-associated dyspareunia: the impact on women’s lives. BMJ Sexual & Reproductive Health, 33(3), 189-193. Retrieved from https://srh.bmj.com/content/familyplanning/33/3/189.full.pdf
Fritzer, N., & Hudelist, G. (2017). Love is a pain? Quality of sex life after surgical resection of endometriosis: a review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 209, 72-76. Retrieved from https://doi.org/10.1016/j.ejogrb.2016.04.036
Orr, N. L., Noga, H., Williams, C., Allaire, C., Bedaiwy, M. A., Lisonkova, S., … & Yong, P. J. (2018). Deep dyspareunia in endometriosis: role of the bladder and pelvic floor. The journal of sexual medicine, 15(8), 1158-1166. DOI: 10.1016/j.jsxm.2018.06.007
Wahl, K. J., Orr, N. L., Lisonek, M., Noga, H., Bedaiwy, M. A., Williams, C., … & Yong, P. J. (2020). Deep dyspareunia, superficial dyspareunia, and infertility concerns among women with endometriosis: a cross-sectional study. Sexual medicine, 8(2), 274-281. Retrieved from https://doi.org/10.1016/j.esxm.2020.01.002
Yong, P. J. (2017). Deep dyspareunia in endometriosis: a proposed framework based on pain mechanisms and genito-pelvic pain penetration disorder. Sexual medicine reviews, 5(4), 495-507. Retrieved from https://doi.org/10.1016/j.sxmr.2017.06.005
Physical Therapy Before Excision Surgery for Endometriosis
Table of contents
- Physical Therapists can Optimize Care by Helping a Patient Get to a Specialist while Providing Physical Therapy Treatment.
- Endo Specialists’ Wait Times Vary Greatly Depending on Where You are Located.
- Most Studies Research the Effectiveness of Physical Therapy Following Excision Surgery. What About Physical Therapy Before Excision Surgery?
- A Few Factors to Keep in Mind if You are Seeking Pelvic Physical Therapy Before Excision Surgery
Endometriosis can cause multiple issues for patients. And it can create the need for a multidisciplinary care team to address chronic pelvic pain. Physical therapy is one example of part of a multidisciplinary treatment plan for endometriosis symptoms. Guest writer Rebecca Patton, PT, DPT, discusses considerations for using physical therapy while awaiting excision surgery:
Pelvic physical therapy has gained more following and prompted much-needed discussions in recent years. However, pelvic physical therapy looks quite different for someone with chronic pelvic pain and endometriosis.
The reality is that pelvic physical therapists may be the first line of defense to refer a patient to a specialist. First, because we have direct access, meaning a patient can see us for an evaluation before seeing a physician. Second, because symptoms of endometriosis are often missed or dismissed by referring providers. In the latter case, someone may be referred to physical therapy before excision surgery or even before seeing an endo specialist.
Physical Therapists can Optimize Care by Helping a Patient Get to a Specialist while Providing Physical Therapy Treatment.
If we are seeking to provide the best care available for the treatment of endo, getting a faster diagnosis and referring a patient to an excision specialist is the primary goal. With a thorough medical history including bowel and bladder habits, menstrual symptoms, pelvic pain symptoms, previous treatment, and understanding the patient’s experience, a pelvic physical therapist can create a differential diagnosis list that may include endometriosis. If endometriosis is suspected, a referral to an excision specialist should be given to the patient and explained.
Endo Specialists’ Wait Times Vary Greatly Depending on Where You are Located.
In my personal experience in Phoenix, AZ, a large metropolitan area with several specialists, it takes anywhere from 3-12 months. More time if we are in the middle of a global pandemic. Decreased access in rural areas may also increase waiting times. One positive change is the inclusion of virtual appointments which may improve access for those in rural areas.
During the waiting period, the goal is to manage pain and maintain some regularity with bowel and bladder habits until excision surgery. Internal pelvic floor retraining may or may not be appropriate during this time.
As mentioned before, physical therapy before excision surgery is going to look different from treatments for other conditions. As a patient, you want to ensure the physical therapist you are seeing treats patients with endo regularly. You may want to consult with them prior about how often they treat patients with endo and what treatments they use specifically. Additional coursework for visceral and abdominal manual therapy techniques, nerve mobilization, and myofascial therapy techniques will be helpful.
Most Studies Research the Effectiveness of Physical Therapy Following Excision Surgery. What About Physical Therapy Before Excision Surgery?
Zhao et al. (1) found that 12 weeks of PMR (progressive muscle relaxation) training is effective in improving anxiety, depression, and quality of life of endometriosis patients under GnRH agonist therapy. These participants had not received excision surgery.
Awad et al. (2) found improvements in posture and pain with an 8-week regular exercise program in those diagnosed with mild to moderate endometriosis. This exercise program included posture awareness, diaphragm breathing, muscle relaxation techniques, lower back and hip stretches, and walking. Of note, this exercise program was not vigorous exercise. These participants were also receiving hormonal treatment but not receiving pain medication.
Both studies did not say that physical exercise or PMR plays a role in the prevention of the occurrence or progression of endometriosis. Both studies were short-term (8-12 weeks) and did not explore pain management directly before excision or outcomes after excision.
In the time that a patient is waiting for excision surgery, I believe physical therapy treatment can be effective at minimizing overall pain levels and improving quality of life.
A Few Factors to Keep in Mind if You are Seeking Pelvic Physical Therapy Before Excision Surgery
1. Your symptoms after physical therapy should not last more than 1-2 days and should feel manageable. Being bedridden for a week after physical therapy is not a helpful treatment. If you experience this, be sure to communicate it with your physical therapist to adjust the plan. Not all pelvic PTs are experienced with this type of treatment and they may create an exercise plan that is too vigorous.
2. Internal pelvic floor treatment is not always the most helpful in this situation and may exacerbate symptoms. An individualized plan is important to discuss with your provider.
3. You are in charge of your body. If you don’t feel like treatment is working then communicate that to your team and discuss other options. It is always okay to voice your concerns to change the treatment to fit you best.
4. Treatment before surgery requires a multidisciplinary team. This may include other pain management options including medication.
iCareBetter is doing the groundwork to vet pelvic physical therapists.
Rebecca Patton PT, DPT (If you are seeking a pelvic PT, I accept consultations through my website for in person and telehealth appointments: https://www.pattonpelvichealth.com/)
For more resources on physical therapy for endometriosis see: https://nancysnookendo.com/learning-library/treatment/lessons/physical-therapy-resources/
References
Zhao L, Wu H, Zhou X, et al.: Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol, 2012, 162: 211–215. [PubMed] [Google Scholar]
Awad E, Ahmed HAH, Yousef A, Abbas R. Efficacy of exercise on pelvic pain and posture associated with endometriosis: within subject design. J Phys Ther Sci. 2017;29(12):2112-2115. doi:10.1589/jpts.29.2112 [NCBI]

Physical Therapy Before Excision Surgery for Endometriosis
Endometriosis can cause multiple issues for our bodies and can create the need for a multidisciplinary care team to address chronic pelvic pain. Physical therapy is one example of part of a multidisciplinary treatment plan for endometriosis symptoms. Guest writer Rebecca Patton, PT, DPT, discusses considerations for using physical therapy while awaiting excision surgery:
Pelvic physical therapy has gained more following and prompted much needed discussions in recent years. However, pelvic physical therapy looks quite different for someone with chronic pelvic pain and endometriosis.
The reality is that pelvic physical therapists may be a first line of defense to refer a patient to a specialist. First, because we have direct access, meaning a patient can see us for an evaluation before seeing a physician. Second, because symptoms of endometriosis are often missed or dismissed by referring providers. In the latter case, someone may be referred to physical therapy before excision surgery or even before seeing an endo specialist.
Top endometriosis physical therapists
Endometriosis Physical Therapy
pelvic floor therapy for endometriosis
Physical therapists can optimize care by helping a patient get to a specialist while providing physical therapy treatment.
If we are seeking to provide the best care available for treatment of endo, getting faster diagnosis and referring a patient to an excision specialist is the primary goal. With a thorough medical history including bowel and bladder habits, menstrual symptoms, pelvic pain symptoms, previous treatment, and understanding the patient’s experience, a pelvic physical therapist can create a differential diagnosis list that may include endometriosis. If endometriosis is suspected, a referral to an excision specialist should be given to the patient and explained.
Endo specialists’ wait times vary greatly depending on where you are located.
In my personal experience in Phoenix, AZ, a large metropolitan area with several specialists, it takes anywhere from 3-12 months. More time if we are in the middle of a global pandemic. Decreased access in rural areas may also increase waiting times. One positive change is the inclusion of virtual appointments which may improve access for those in rural areas.
During the waiting period, the goal is to manage pain and maintain some regularity with bowel and bladder habits until excision surgery. Internal pelvic floor retraining may or may not be appropriate during this time.
As mentioned before, physical therapy before excision surgery is going to look different from treatments for other conditions. As a patient, you want to ensure the physical therapist you are seeing treats patients with endo regularly. You may want to consult with them prior about how often they treat patients with endo and what treatments they use specifically. Additional coursework for visceral and abdominal manual therapy techniques, nerve mobilization, and myofascial therapy techniques will be helpful.
Most studies research the effectiveness of physical therapy following excision surgery. What about physical therapy before excision surgery?
Zhao et al. (1) found that 12 weeks of PMR (progressive muscle relaxation) training is effective in improving anxiety, depression and QOL of endometriosis patients under GnRH agonist therapy. These participants had not received excision surgery.
Awad et al. (2) found improvements in posture and pain with an 8-week regular exercise program in those diagnosed with mild to moderate endometriosis. This exercise program included posture awareness, diaphragm breathing, muscle relaxation techniques, lower back and hip stretches, and walking. Of note, this exercise program was not vigorous exercise. These participants were also receiving hormonal treatment but not receiving pain medication.
Both studies did not say that physical exercise or PMR plays a role in the prevention of the occurrence or progression of endometriosis. Both studies were short term (8-12 weeks) and did not explore pain management directly before excision or outcomes after excision.
In the time that a patient is waiting for excision surgery, I believe physical therapy treatment can be effective at minimizing overall pain levels and improving quality of life.
A few factors to keep in mind if you are seeking pelvic physical therapy before excision surgery:
- Your symptoms after physical therapy should not last more than 1-2 days and should feel manageable. Being bedridden for a week after physical therapy is not a helpful treatment. If you experience this, be sure to communicate it with your physical therapist to adjust the plan. Not all pelvic PT’s are experienced with this type of treatment and they may create an exercise plan that is too vigorous.
- Internal pelvic floor treatment is not always the most helpful in this situation and may exacerbate symptoms. An individualized plan is important to discuss with your provider.
- You are in charge of your body. If you don’t feel like a treatment is working then communicate that to your team and discuss other options. It is always okay to voice your concerns to change the treatment to fit you best.
- Treatment before surgery requires a multidisciplinary team. This may include other pain management options including medication.
iCareBetter is doing the ground work to vet pelvic physical therapists.
Rebecca Patton PT, DPT (If you are seeking a pelvic PT, I accept consultations through my website for in person and telehealth appointments: https://www.pattonpelvichealth.com/)
For more resources on physical therapy for endometriosis see: https://icarebetter.com/physical-therapy-resources/
References
Zhao L, Wu H, Zhou X, et al.: Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol, 2012, 162: 211–215. [PubMed] [Google Scholar]
Awad E, Ahmed HAH, Yousef A, Abbas R. Efficacy of exercise on pelvic pain and posture associated with endometriosis: within subject design. J Phys Ther Sci. 2017;29(12):2112-2115. doi:10.1589/jpts.29.2112 [NCBI]

Choosing the Right Mental Health Therapist
By Deanna Denman, PhD, Licensed Psychologist, Clinical Health Psychologist
Find the right therapist can be just as difficult as finding an endometriosis specialist. There are many different types of therapists providing many different types of therapy out there, and “fit” between you and your therapist is very important. I’ve included some helpful information and tips below to help you find a good therapist if you’d like some support along your Endo journey.
- Finding a therapist-
-Expect to check out several therapists via website. Most therapists offer a free consultation to see if you both think it’s a good fit. The “fit” with you and your therapist is going to be important for your trust and ultimately your progress in therapy.
-If you meet with someone and they aren’t a good fit, that’s okay! You can even ask them if they have referrals for you.
-Ask your doctor if they have any recommendations. Some doctors have therapists they have worked with in the past and who they trust. Ask if your doctor has any referrals for you.
-There are SEVERAL therapist directories. Search them for therapists in your area. I encourage you to check out:
- Inclusive Therapists
- Psychology Today
- Therapy for Black Girls
- Therapy for Latinx
- QTPOC
- Your insurance company (they usually list covered providers on their website)
- Your network (friends, family, co-workers) if you are comfortable
**Some people prefer to work with therapists who hold similar identities to them. I’ve included some resources for therapists of color and LGBTQ+ therapists in the list above***
2. What to ask-
So you’ve found a few potential therapists. What should you ask in the first consultation:
-How much do sessions cost?
Therapy is an investment in your well-being, but I know costs can be prohibitive! BE thoughtful and open about your budget for therapy. Many therapists list their rates online as well as whether or not they accept insurance. Some therapists don’t accept insurance, but will still provide you with a receipt for services that you can provide to your insurance for reimbursement. ***Talk to your insurance provider about your out-of-network mental health benefits.***
-How much experience and what trainings do you have in working with people with endometriosis?
(You can also ask about other things you’d like to work on in therapy like trauma, anxiety, or even people-pleasing). Really anything is fair game, but it’s important to assess their comfort level with your particular concerns. Specifically, if you are seeking support with your Endo, you want to know if they are familiar with the condition, if they are comfortable in collaborating with your medical providers, and what kinds of interventions they use. If they have never worked with someone with chronic pain, or their only recommendation for someone with chronic pain is to start exercising, they’re not likely to be a good fit.
–How will we set goals/measure progress?
Ideally, you want to set goals together with your therapist. You should also check in regularly about how you are doing and the plan for moving forward
3. Credentials-
If you’ve ever been confused by the alphabet soup after therapists’ names, you’re not alone. The conversation around the differences between “counseling” and “therapy” are beyond the scope of this post. Most people use the terms interchangeably and the right provider for you could fall into either category.
***Note: any provider you work with must be licensed to practice (or pursuing licensure and working under supervision)***
Let’s break it down:
Professional Counselors
- LPC- licensed professional counselor (may have -A, -S behind LPC to designate “associate” or “supervisor”)
- LMHC- licensed mental health counselor
- LCADAC- licensed clinical alcohol and drug abuse counselor
- LMFT- licensed marriage and family therapist
Broadly, counselors are more focused on helping you solve mental health and behavioral problems and giving you very practical skills.
*LMFTs are not technically counselors (their title even includes ‘therapist’), but they best fit in this category, and tend to specialize in things influenced by relationships. LMFTs DO offer individual therapy and often have specialty training in concerns like infertility.
Social Workers
- LCSW- licensed clinical social worker (may have -A, or -C behind LCSW to designate “associate” or “certified”)
- LISW- licensed independent social worker
- MSW- Master of social work (the degree)
Again, broadly, social workers are very well trained to address social and environmental issues (think: systems of oppression and “isms”) and problem-solve. They also tend to be very knowledgeable about resources (like programs and trainings) that can help you.
Psychologists
- PhD- doctor of philosophy
- PsyD- doctor of psychology
Generally, psychologists focus on very complex issues and very strongly grounded in theories of mental health. They tend to be more assessment-, and research-, focused due to their training. (They can also do psychological testing for things like memory and learning disabilities)
These are all very broad generalizations and still don’t address people’s specialties (the populations they focus on), the theory they are grounded in, or the interventions they use. The best place to get a sense of that is by reading their websites and speaking with them directly.
What’s important- regardless of the letters, most of them are trained to help people work things out in therapy. They will NOT all have the training to help with issues around endometriosis. That’s why taking advantage of the consultation is important.
4. Specialties-
Therapists often have specialties. Realistically, you can find therapists specializing in just about anything. There are some therapists who specialize in trauma, others who specialize in working with high-achievers who want to slow down. There are ALSO therapists who specialize in working with patients who have chronic illness. You may want to see a provider who has specialty training and focus in working with patients with chronic illness. Finding the right therapist for you can take some effort but is worth it. Consider what you’d like to address and look for therapists who speak to that on their sites/listings. If you can, take advantage of free consultations. Ask potential therapists about their experience and training in your concerns. Be open to trying more than one and know that personality fit is important. It’s okay to search until you find the right support for you on this endometriosis journey.
