

What are the First Signs and Symptoms of Endometriosis: Everything You Need to Know
Table of contents
- What is the Endometrium?
- What is Endometriosis Pain?
- Mechanisms of Signs and Symptoms of Endometriosis :
- Painful Periods (dysmenorrhea)
- Diarrhea During Menstrual Periods
- Pain During Intercourse (Dyspareunia)
- Abdominal or Pelvic Pain After Vaginal Sex
- Painful Urination During or Between Menstrual Periods (Dysuria)
- Painful Bowel Movements During or Between Menstrual Periods (Dyschezia)
- Gastrointestinal Problems, Including Bloating, Diarrhea, Constipation, and Nausea
- Causes of Endometriosis
- Complications of Endometriosis
- Diagnosis of Endometriosis
- Treatment for Endometriosis
- Surgical Treatment Options for Endometriosis:
- Multidisciplinary Care
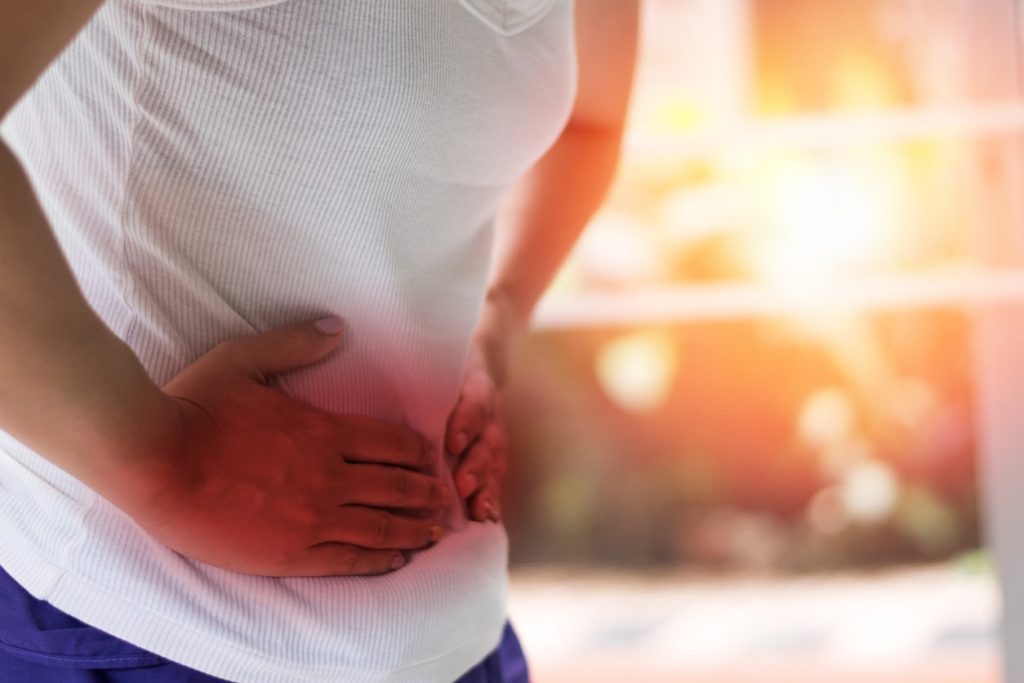
Sharp. Stabbing. Burning. Throbbing. Aching. All these adjectives have been used to describe endometriosis pain. Endometriosis is a condition that, for some women, can cause excruciating uterus pain. Some describe it as feeling like their insides are being pulled out of their bodies. Even worse – endometriosis pain medication doesn’t cut through or provide relief for many patients with this condition. Therefore, an endometriosis diagnosis can be very serious and life-changing news.
Our commitment to our patients runs deep, and our mission is to help patients with endometriosis pain and other complications find the skilled doctors they need.
As our first introduction to the disorder, we will give you a brief overview of the signs and symptoms of endometriosis, its causes, complications, and treatment options (or, as we like to call it – hope). First, we will give you general information on the disease and cover what endometriosis is.
What is the Endometrium?
The endometrium, also known as the endometrial lining, is the tissue that comprises the “wallpaper”, or lining of the uterus. The uterus is the pear-shaped organ that houses a growing baby. During pregnancy and menstruation, the endometrium plays vital functions.
What is Endometriosis Pain?
Endometriosis is pronounced (en-doe-me-tree-O-sis). Endometriosis is a medical condition in which tissue similar to what normally lines the inner walls of the uterus, also known as the endometrium, grows outside the uterus. It is often a very painful, even debilitating disorder. It may involve the ovaries, fallopian tubes, bowels, vagina, cervix, and the tissues that line the pelvis. In rare cases, it can also affect other organs, such as the bladder, kidneys, or lungs.
Signs and Symptoms of Endometriosis Pain
Not all women will experience the same symptoms of endometriosis or degree of intensity/severity. Some women may not experience any symptoms at all.
It is also important to keep in mind that the severity of symptoms is not a solid indicator of the progress of the disease. There are women with advanced stages of endometriosis who experience no symptoms at all and others with mild cases who endure many. Common endometriosis pain symptoms include:
- Painful periods, or dysmenorrhea
- Infertility
- Diarrhea during period
- Pain during intercourse
- Heavy or abnormal menstrual flow
- Abdominal or pelvic pain after vaginal sex
- Painful urination during or between menstrual periods
- Painful bowel movements during or between menstrual periods
- Gastrointestinal problems, including bloating, diarrhea, constipation, and/or nausea
Mechanisms of Signs and Symptoms of Endometriosis:
Painful Periods (dysmenorrhea)
Cyclic release of multiple inflammatory factors activates nerve fiber growth, leads to cell damage and fibrosis, and exacerbates pain during periods.
Infertility
The overall mechanisms can include tubal blockage, local inflammation, uterine muscle dysfunction, local hormonal alterations, and much more.
Diarrhea During Menstrual Periods
Diarrhea may result from endometriosis growing directly on the rectal muscle or endometriosis inflammatory substances. Local production of inflammatory molecules can lead to hyper-motility of the sigmoid and rectum muscles, which can manifest as cramping and diarrhea.
Pain During Intercourse (Dyspareunia)
Endometriosis implants have more nerve endings than usual (hyperinnervated) and can produce pain with pressure. The act of intercourse can apply this pressure on the upper vaginal area and uterosacral ligaments, which are common locations of endo implants. Once this pain occurs and local inflammation further causes tension in the pelvic floor, the muscles surrounding the vagina can contract, which worsens the problem.
Heavy or abnormal menstrual flow
Endometriosis can impact your bleeding by increasing stress from pain or damage to the ovaries, which can change local hormonal function.
Abdominal or Pelvic Pain After Vaginal Sex
Uterine and pelvic floor spasms are part of regular orgasms. When these areas are hypersensitive due to endometriosis, spasms lead to continued contractions and pain that lasts for a while. In addition, rectal fusion to the posterior vaginal wall will also cause more direct pain and inflammation by the vaginal area pulling on the rectal wall. Also, as you probably recognize, any event that stirs up the pelvis and causes some trauma leads to increased molecular signaling, further amplifying the problem.
Painful Urination During or Between Menstrual Periods (Dysuria)
Painful and frequent urination is a prevalent symptom of endometriosis. Endo cells and responding inflammatory cells produce inflammatory molecular signals that aggregate in the area of injury. These molecular signals affect all pelvic organs, including the bladder, leading to bladder wall spasms. Moreover, interstitial cystitis is common in endometriosis patients and can also be a factor. In the worst-case scenario, endo lesions implant inside the bladder, which can also cause cyclic bleeding from the bladder (hematuria).
Painful Bowel Movements During or Between Menstrual Periods (Dyschezia)
Endometriosis causes inflammation and fibrosis or scarring as your body attempts to heal. This inflammation and fibrosis can severely alter the anatomy in the pelvis and distort the rectal course, gluing it to the uterus, cervix, and posterior vaginal wall. This angulation can cause constipation and trouble evacuating stool, while the inflammatory signals cause the rectal muscles to hyper-contract. These mechanisms lead to painful bowel movements, which worsen during the cyclic increases in inflammatory molecules. In the worst-case scenario, the endo will grow through the rectum wall over time, causing cyclic rectal bleeding.
Gastrointestinal Problems, Including Bloating, Diarrhea, Constipation, and Nausea
Generally, intestinal symptoms of endometriosis can be direct or indirect or related to conditions like small intestinal bacterial overgrowth (SIBO). Even if there are no direct implants on the bowel, the endo inside the abdomen and pelvis can cause enough inflammation to irritate the intestine and cause symptoms. In addition, endometriosis implants directly on the bowel can worsen the symptoms.
Causes of Endometriosis
One cause of endometriosis is the direct transplantation of endometrial cells into the abdominal wall during a medical procedure, such as a cesarean section. Besides this known cause of endometriosis, other theories exist as to how it develops:
1. One theory is that during the menstrual cycle, a reverse process takes place where the tissue backs up through the fallopian tubes and into the abdominal cavity, where it attaches and grows.
2. Another theory is a genetic link. This is based on studies that show if someone has a family member with endometriosis, they are more likely to have it as well.
3. Some also suggest that the endometrial tissues travel and implant in other body parts via blood or lymphatic channels, like cancer cells spread.
4. A fourth theory suggests that all cells throughout the body have the ability to transform into endometrial cells.
Complications of Endometriosis
The following are complications of endometriosis if left untreated or in advanced stages of the disorder:
- Infertility/subfertility
- Chronic pelvic pain that can result in disability
- Anatomic disruption of involved organ systems (i.e., adhesions, ruptured cysts, renal failure)
Diagnosis of Endometriosis
The diagnosis starts with assessing signs and symptoms and then performing imaging studies such as MRI and ultrasonography. But the confirmation or exclusion of the endometriosis diagnosis is only possible with surgical biopsy and histopathology. Laparoscopy is the gold-standard surgical modality for diagnosis in all cases.
Treatment for Endometriosis
Endometriosis needs a multidisciplinary team approach for effective and holistic treatment. This team should include the following medical professionals:
- Nutritionist
- Physical therapist
- Endometriosis surgeon
- Mental health therapist
- Pain management specialist
Pain is often the biggest complaint from patients with endometriosis. Therefore, many treatment options are aimed at pain control. So first, here are some options for women to help temporarily ease the pain of endometriosis:
- Exercise
- Meditation
- Breath work
- Heating pads
- Rest and relaxation
- Prevention of constipation
These therapies may be used in combination with medical and/or surgical options to lessen the pelvic pain associated with this disorder. Furthermore, alternative therapies exist that may be used in conjunction with other interventions, and those include but are not limited to:
- Homeopathy
- Immune therapy
- Allergy management
- Nutritional approached
- Traditional Chinese medicine
*Be sure to discuss any of these treatment options with a physician before implementing them.
The Right Medical Treatment For You:
Options for medical and/or surgical treatments for endometriosis are going to depend on several factors, including:
- Desire for pregnancy
- The extent of the disease
- Type and severity of symptoms
- Patient opinions and preferences
- Overall health and medical history
- Expectations of the course of the disease
- Patients’ tolerance level for medications, therapies, and/or procedures
In some cases, management of pain might be the only treatment. In others, medical options may be considered. The following are typical non-surgical, medical treatments for endometriosis:
- “Watch and Wait” approach, where the course of the disease is monitored and treated accordingly
- Pain medication (anything from non-steroidal anti-inflammatory drugs [NSAIDs] to other over-the-counter and/or prescription analgesics)
- Hormonal therapy, such as:
- Progestins
- Oral contraceptives with both estrogen and progestin to reduce menstrual flow and block ovulation
- Danazol (a synthetic derivative of the male hormone testosterone)
- Gonadotropin-releasing hormone antagonist, which stops ovarian hormone production
Surgical Treatment Options for Endometriosis:
Despite their effectiveness in symptom control, pain medications can have significant side effects. Moreover, these medications do not stop the progression of the disease, and symptoms might return once stopped. But on the other side, surgery can lead to long-term relief and can prevent further damage to tissues. Your treatment plan should be a shared decision based on your desires, goals, and abilities.
Almost all endometriosis surgical procedures are laparoscopic or robotic. These are minimally invasive surgeries in which small tubes with lights and cameras are inserted into the abdominal wall. It allows the doctor to see the internal organs and remove endometriosis.
Excision of Endometriosis
In this technique, a surgeon cuts out much or all of the endometriosis lesions from the body. Therefore, surgeons avoid leaving any endometriosis lesions behind while preserving normal tissues. This technique is widely adopted by highly skilled endometriosis surgeons who are world leaders.
Ablation of Endometriosis
In this technique, a surgeon burns the surface of the endometriosis lesions and leaves them in the body. Most top experts highly criticize this ablation method. Ablation is most popular with surgeons who have not received enough training to do excision. As a result, these surgeons are not comfortable performing excision, and they do the ablation.
Hysterectomy
this is a surgery in which surgeons remove the uterus and sometimes ovaries. But, many surgeons consider hysterectomy an outdated and ineffective treatment for endometriosis. Almost all top endometriosis surgeons reject doing it unless there is a clear indication for hysterectomy such as adenomyosis.
Laparotomy
this surgical procedure cuts and opens the abdomen and does not use thin tubes. Therefore it is more extensive than a laparoscopy. Very few surgeons still do laparotomy because of its complications. Almost none of the top endometriosis surgeons do laparotomy for endometriosis.
Multidisciplinary Care
Along with effective surgical treatment, the patient should start working with endometriosis experts in physical therapy, mental health, nutrition, and pain management to achieve the best possible outcome.
Get in touch with Dr. Steve Vasilev

Pain with sex
A little spoken of symptom of endometriosis is pain with sex. In medical terms, it is called dyspareunia- meaning pelvic pain that occurs before, during, or after intercourse (although similar pain can also be felt with an exam or insertion of a tampon). Deep dyspareunia is “a cardinal symptom of endometriosis” (Wahl et al., 2020) with more than half of women with endometriosis experiencing it (Yong, 2017). This can play a significant role in the quality of life and relationships (Denny & Mann, 2007). The pain has been described cramping, stabbing, or stinging- among other things.
Yong (2017) proposes a classification of four types of deep dyspareunia in people with endometriosis: “type I that is directly due to endometriosis; type II that is related to a comorbid condition; type III in which genito-pelvic pain penetration disorder is primary; and type IV that is secondary to a combination of types I to III.” Fritzer and Hudelist (2017) found that “surgical excision of endometriosis is a feasible and good treatment option for pain relief and improvement of quality of sex life in symptomatic women with endometriosis.” Excision surgery for endometriosis overall shows improvement in pain with sex; however, other factors such as adenomyosis or painful bladder syndrome (interstitial cystitis) can continue to cause symptoms and should be addressed (Crispi et al., 2021). “Myofascial or nervous system mechanisms may be important for deep dyspareunia in women with endometriosis, even in those with moderate-to-severe disease (Stage III/IV)” (Orr et al., 2018). While it may feel embarrassing to bring up, it is an important aspect of your health to discuss with your provider. They might suggest pelvic floor therapy, medication, or other options to help. But it is important to address any underlying conditions.
In the meantime, some things to try:
- Have open communication with your partner about what you are feeling and your needs
- Experiment with different times of your cycle that may be less painful (such as the week after ovulation or the first couple of weeks after your period)
- Use of a lubricant
- Try different positions to find which is best for you
- Utilizing forms of intimacy that does not involve penetration
Find more here: https://icarebetter.com/pain-with-penetration/
References
Crispi Jr, C. P., Crispi, C. P., de Oliveira, B. R. S., de Nadai Filho, N., Peixoto-Filho, F. M., & Fonseca, M. D. F. (2021). Six-month follow-up of minimally invasive nerve-sparing complete excision of endometriosis: What about dyspareunia?. Plos one, 16(4), e0250046. Retrieved from https://doi.org/10.1371/journal.pone.0250046
Denny, E., & Mann, C. H. (2007). Endometriosis-associated dyspareunia: the impact on women’s lives. BMJ Sexual & Reproductive Health, 33(3), 189-193. Retrieved from https://srh.bmj.com/content/familyplanning/33/3/189.full.pdf
Fritzer, N., & Hudelist, G. (2017). Love is a pain? Quality of sex life after surgical resection of endometriosis: a review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 209, 72-76. Retrieved from https://doi.org/10.1016/j.ejogrb.2016.04.036
Orr, N. L., Noga, H., Williams, C., Allaire, C., Bedaiwy, M. A., Lisonkova, S., … & Yong, P. J. (2018). Deep dyspareunia in endometriosis: role of the bladder and pelvic floor. The journal of sexual medicine, 15(8), 1158-1166. DOI: 10.1016/j.jsxm.2018.06.007
Wahl, K. J., Orr, N. L., Lisonek, M., Noga, H., Bedaiwy, M. A., Williams, C., … & Yong, P. J. (2020). Deep dyspareunia, superficial dyspareunia, and infertility concerns among women with endometriosis: a cross-sectional study. Sexual medicine, 8(2), 274-281. Retrieved from https://doi.org/10.1016/j.esxm.2020.01.002
Yong, P. J. (2017). Deep dyspareunia in endometriosis: a proposed framework based on pain mechanisms and genito-pelvic pain penetration disorder. Sexual medicine reviews, 5(4), 495-507. Retrieved from https://doi.org/10.1016/j.sxmr.2017.06.005
Physical Therapy Before Excision Surgery for Endometriosis
Table of contents
- Physical Therapists can Optimize Care by Helping a Patient Get to a Specialist while Providing Physical Therapy Treatment.
- Endo Specialists’ Wait Times Vary Greatly Depending on Where You are Located.
- Most Studies Research the Effectiveness of Physical Therapy Following Excision Surgery. What About Physical Therapy Before Excision Surgery?
- A Few Factors to Keep in Mind if You are Seeking Pelvic Physical Therapy Before Excision Surgery
Endometriosis can cause multiple issues for patients. And it can create the need for a multidisciplinary care team to address chronic pelvic pain. Physical therapy is one example of part of a multidisciplinary treatment plan for endometriosis symptoms. Guest writer Rebecca Patton, PT, DPT, discusses considerations for using physical therapy while awaiting excision surgery:
Pelvic physical therapy has gained more following and prompted much-needed discussions in recent years. However, pelvic physical therapy looks quite different for someone with chronic pelvic pain and endometriosis.
The reality is that pelvic physical therapists may be the first line of defense to refer a patient to a specialist. First, because we have direct access, meaning a patient can see us for an evaluation before seeing a physician. Second, because symptoms of endometriosis are often missed or dismissed by referring providers. In the latter case, someone may be referred to physical therapy before excision surgery or even before seeing an endo specialist.
Physical Therapists can Optimize Care by Helping a Patient Get to a Specialist while Providing Physical Therapy Treatment.
If we are seeking to provide the best care available for the treatment of endo, getting a faster diagnosis and referring a patient to an excision specialist is the primary goal. With a thorough medical history including bowel and bladder habits, menstrual symptoms, pelvic pain symptoms, previous treatment, and understanding the patient’s experience, a pelvic physical therapist can create a differential diagnosis list that may include endometriosis. If endometriosis is suspected, a referral to an excision specialist should be given to the patient and explained.
Endo Specialists’ Wait Times Vary Greatly Depending on Where You are Located.
In my personal experience in Phoenix, AZ, a large metropolitan area with several specialists, it takes anywhere from 3-12 months. More time if we are in the middle of a global pandemic. Decreased access in rural areas may also increase waiting times. One positive change is the inclusion of virtual appointments which may improve access for those in rural areas.
During the waiting period, the goal is to manage pain and maintain some regularity with bowel and bladder habits until excision surgery. Internal pelvic floor retraining may or may not be appropriate during this time.
As mentioned before, physical therapy before excision surgery is going to look different from treatments for other conditions. As a patient, you want to ensure the physical therapist you are seeing treats patients with endo regularly. You may want to consult with them prior about how often they treat patients with endo and what treatments they use specifically. Additional coursework for visceral and abdominal manual therapy techniques, nerve mobilization, and myofascial therapy techniques will be helpful.
Most Studies Research the Effectiveness of Physical Therapy Following Excision Surgery. What About Physical Therapy Before Excision Surgery?
Zhao et al. (1) found that 12 weeks of PMR (progressive muscle relaxation) training is effective in improving anxiety, depression, and quality of life of endometriosis patients under GnRH agonist therapy. These participants had not received excision surgery.
Awad et al. (2) found improvements in posture and pain with an 8-week regular exercise program in those diagnosed with mild to moderate endometriosis. This exercise program included posture awareness, diaphragm breathing, muscle relaxation techniques, lower back and hip stretches, and walking. Of note, this exercise program was not vigorous exercise. These participants were also receiving hormonal treatment but not receiving pain medication.
Both studies did not say that physical exercise or PMR plays a role in the prevention of the occurrence or progression of endometriosis. Both studies were short-term (8-12 weeks) and did not explore pain management directly before excision or outcomes after excision.
In the time that a patient is waiting for excision surgery, I believe physical therapy treatment can be effective at minimizing overall pain levels and improving quality of life.
A Few Factors to Keep in Mind if You are Seeking Pelvic Physical Therapy Before Excision Surgery
1. Your symptoms after physical therapy should not last more than 1-2 days and should feel manageable. Being bedridden for a week after physical therapy is not a helpful treatment. If you experience this, be sure to communicate it with your physical therapist to adjust the plan. Not all pelvic PTs are experienced with this type of treatment and they may create an exercise plan that is too vigorous.
2. Internal pelvic floor treatment is not always the most helpful in this situation and may exacerbate symptoms. An individualized plan is important to discuss with your provider.
3. You are in charge of your body. If you don’t feel like treatment is working then communicate that to your team and discuss other options. It is always okay to voice your concerns to change the treatment to fit you best.
4. Treatment before surgery requires a multidisciplinary team. This may include other pain management options including medication.
iCareBetter is doing the groundwork to vet pelvic physical therapists.
Rebecca Patton PT, DPT (If you are seeking a pelvic PT, I accept consultations through my website for in person and telehealth appointments: https://www.pattonpelvichealth.com/)
For more resources on physical therapy for endometriosis see: https://nancysnookendo.com/learning-library/treatment/lessons/physical-therapy-resources/
References
Zhao L, Wu H, Zhou X, et al.: Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol, 2012, 162: 211–215. [PubMed] [Google Scholar]
Awad E, Ahmed HAH, Yousef A, Abbas R. Efficacy of exercise on pelvic pain and posture associated with endometriosis: within subject design. J Phys Ther Sci. 2017;29(12):2112-2115. doi:10.1589/jpts.29.2112 [NCBI]

Physical Therapy Before Excision Surgery for Endometriosis
Endometriosis can cause multiple issues for our bodies and can create the need for a multidisciplinary care team to address chronic pelvic pain. Physical therapy is one example of part of a multidisciplinary treatment plan for endometriosis symptoms. Guest writer Rebecca Patton, PT, DPT, discusses considerations for using physical therapy while awaiting excision surgery:
Pelvic physical therapy has gained more following and prompted much needed discussions in recent years. However, pelvic physical therapy looks quite different for someone with chronic pelvic pain and endometriosis.
The reality is that pelvic physical therapists may be a first line of defense to refer a patient to a specialist. First, because we have direct access, meaning a patient can see us for an evaluation before seeing a physician. Second, because symptoms of endometriosis are often missed or dismissed by referring providers. In the latter case, someone may be referred to physical therapy before excision surgery or even before seeing an endo specialist.
Top endometriosis physical therapists
Endometriosis Physical Therapy
pelvic floor therapy for endometriosis
Physical therapists can optimize care by helping a patient get to a specialist while providing physical therapy treatment.
If we are seeking to provide the best care available for treatment of endo, getting faster diagnosis and referring a patient to an excision specialist is the primary goal. With a thorough medical history including bowel and bladder habits, menstrual symptoms, pelvic pain symptoms, previous treatment, and understanding the patient’s experience, a pelvic physical therapist can create a differential diagnosis list that may include endometriosis. If endometriosis is suspected, a referral to an excision specialist should be given to the patient and explained.
Endo specialists’ wait times vary greatly depending on where you are located.
In my personal experience in Phoenix, AZ, a large metropolitan area with several specialists, it takes anywhere from 3-12 months. More time if we are in the middle of a global pandemic. Decreased access in rural areas may also increase waiting times. One positive change is the inclusion of virtual appointments which may improve access for those in rural areas.
During the waiting period, the goal is to manage pain and maintain some regularity with bowel and bladder habits until excision surgery. Internal pelvic floor retraining may or may not be appropriate during this time.
As mentioned before, physical therapy before excision surgery is going to look different from treatments for other conditions. As a patient, you want to ensure the physical therapist you are seeing treats patients with endo regularly. You may want to consult with them prior about how often they treat patients with endo and what treatments they use specifically. Additional coursework for visceral and abdominal manual therapy techniques, nerve mobilization, and myofascial therapy techniques will be helpful.
Most studies research the effectiveness of physical therapy following excision surgery. What about physical therapy before excision surgery?
Zhao et al. (1) found that 12 weeks of PMR (progressive muscle relaxation) training is effective in improving anxiety, depression and QOL of endometriosis patients under GnRH agonist therapy. These participants had not received excision surgery.
Awad et al. (2) found improvements in posture and pain with an 8-week regular exercise program in those diagnosed with mild to moderate endometriosis. This exercise program included posture awareness, diaphragm breathing, muscle relaxation techniques, lower back and hip stretches, and walking. Of note, this exercise program was not vigorous exercise. These participants were also receiving hormonal treatment but not receiving pain medication.
Both studies did not say that physical exercise or PMR plays a role in the prevention of the occurrence or progression of endometriosis. Both studies were short term (8-12 weeks) and did not explore pain management directly before excision or outcomes after excision.
In the time that a patient is waiting for excision surgery, I believe physical therapy treatment can be effective at minimizing overall pain levels and improving quality of life.
A few factors to keep in mind if you are seeking pelvic physical therapy before excision surgery:
- Your symptoms after physical therapy should not last more than 1-2 days and should feel manageable. Being bedridden for a week after physical therapy is not a helpful treatment. If you experience this, be sure to communicate it with your physical therapist to adjust the plan. Not all pelvic PT’s are experienced with this type of treatment and they may create an exercise plan that is too vigorous.
- Internal pelvic floor treatment is not always the most helpful in this situation and may exacerbate symptoms. An individualized plan is important to discuss with your provider.
- You are in charge of your body. If you don’t feel like a treatment is working then communicate that to your team and discuss other options. It is always okay to voice your concerns to change the treatment to fit you best.
- Treatment before surgery requires a multidisciplinary team. This may include other pain management options including medication.
iCareBetter is doing the ground work to vet pelvic physical therapists.
Rebecca Patton PT, DPT (If you are seeking a pelvic PT, I accept consultations through my website for in person and telehealth appointments: https://www.pattonpelvichealth.com/)
For more resources on physical therapy for endometriosis see: https://icarebetter.com/physical-therapy-resources/
References
Zhao L, Wu H, Zhou X, et al.: Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol, 2012, 162: 211–215. [PubMed] [Google Scholar]
Awad E, Ahmed HAH, Yousef A, Abbas R. Efficacy of exercise on pelvic pain and posture associated with endometriosis: within subject design. J Phys Ther Sci. 2017;29(12):2112-2115. doi:10.1589/jpts.29.2112 [NCBI]

Choosing the Right Mental Health Therapist
By Deanna Denman, PhD, Licensed Psychologist, Clinical Health Psychologist
Find the right therapist can be just as difficult as finding an endometriosis specialist. There are many different types of therapists providing many different types of therapy out there, and “fit” between you and your therapist is very important. I’ve included some helpful information and tips below to help you find a good therapist if you’d like some support along your Endo journey.
- Finding a therapist-
-Expect to check out several therapists via website. Most therapists offer a free consultation to see if you both think it’s a good fit. The “fit” with you and your therapist is going to be important for your trust and ultimately your progress in therapy.
-If you meet with someone and they aren’t a good fit, that’s okay! You can even ask them if they have referrals for you.
-Ask your doctor if they have any recommendations. Some doctors have therapists they have worked with in the past and who they trust. Ask if your doctor has any referrals for you.
-There are SEVERAL therapist directories. Search them for therapists in your area. I encourage you to check out:
- Inclusive Therapists
- Psychology Today
- Therapy for Black Girls
- Therapy for Latinx
- QTPOC
- Your insurance company (they usually list covered providers on their website)
- Your network (friends, family, co-workers) if you are comfortable
**Some people prefer to work with therapists who hold similar identities to them. I’ve included some resources for therapists of color and LGBTQ+ therapists in the list above***
2. What to ask-
So you’ve found a few potential therapists. What should you ask in the first consultation:
-How much do sessions cost?
Therapy is an investment in your well-being, but I know costs can be prohibitive! BE thoughtful and open about your budget for therapy. Many therapists list their rates online as well as whether or not they accept insurance. Some therapists don’t accept insurance, but will still provide you with a receipt for services that you can provide to your insurance for reimbursement. ***Talk to your insurance provider about your out-of-network mental health benefits.***
-How much experience and what trainings do you have in working with people with endometriosis?
(You can also ask about other things you’d like to work on in therapy like trauma, anxiety, or even people-pleasing). Really anything is fair game, but it’s important to assess their comfort level with your particular concerns. Specifically, if you are seeking support with your Endo, you want to know if they are familiar with the condition, if they are comfortable in collaborating with your medical providers, and what kinds of interventions they use. If they have never worked with someone with chronic pain, or their only recommendation for someone with chronic pain is to start exercising, they’re not likely to be a good fit.
–How will we set goals/measure progress?
Ideally, you want to set goals together with your therapist. You should also check in regularly about how you are doing and the plan for moving forward
3. Credentials-
If you’ve ever been confused by the alphabet soup after therapists’ names, you’re not alone. The conversation around the differences between “counseling” and “therapy” are beyond the scope of this post. Most people use the terms interchangeably and the right provider for you could fall into either category.
***Note: any provider you work with must be licensed to practice (or pursuing licensure and working under supervision)***
Let’s break it down:
Professional Counselors
- LPC- licensed professional counselor (may have -A, -S behind LPC to designate “associate” or “supervisor”)
- LMHC- licensed mental health counselor
- LCADAC- licensed clinical alcohol and drug abuse counselor
- LMFT- licensed marriage and family therapist
Broadly, counselors are more focused on helping you solve mental health and behavioral problems and giving you very practical skills.
*LMFTs are not technically counselors (their title even includes ‘therapist’), but they best fit in this category, and tend to specialize in things influenced by relationships. LMFTs DO offer individual therapy and often have specialty training in concerns like infertility.
Social Workers
- LCSW- licensed clinical social worker (may have -A, or -C behind LCSW to designate “associate” or “certified”)
- LISW- licensed independent social worker
- MSW- Master of social work (the degree)
Again, broadly, social workers are very well trained to address social and environmental issues (think: systems of oppression and “isms”) and problem-solve. They also tend to be very knowledgeable about resources (like programs and trainings) that can help you.
Psychologists
- PhD- doctor of philosophy
- PsyD- doctor of psychology
Generally, psychologists focus on very complex issues and very strongly grounded in theories of mental health. They tend to be more assessment-, and research-, focused due to their training. (They can also do psychological testing for things like memory and learning disabilities)
These are all very broad generalizations and still don’t address people’s specialties (the populations they focus on), the theory they are grounded in, or the interventions they use. The best place to get a sense of that is by reading their websites and speaking with them directly.
What’s important- regardless of the letters, most of them are trained to help people work things out in therapy. They will NOT all have the training to help with issues around endometriosis. That’s why taking advantage of the consultation is important.
4. Specialties-
Therapists often have specialties. Realistically, you can find therapists specializing in just about anything. There are some therapists who specialize in trauma, others who specialize in working with high-achievers who want to slow down. There are ALSO therapists who specialize in working with patients who have chronic illness. You may want to see a provider who has specialty training and focus in working with patients with chronic illness. Finding the right therapist for you can take some effort but is worth it. Consider what you’d like to address and look for therapists who speak to that on their sites/listings. If you can, take advantage of free consultations. Ask potential therapists about their experience and training in your concerns. Be open to trying more than one and know that personality fit is important. It’s okay to search until you find the right support for you on this endometriosis journey.
Endo diet: Mediterranean or FODMAP for the win?
A healthy eating pattern can be therapeutic and good for our health overall, but it can be difficult to decide on what is best for our bodies. The process can involve a long time spent in trial and error to find what works for our individual body and its needs. When looking at studies on dietary interventions, we find that they are difficult to perform- often ending up with strong bias or high inconsistent rates with adherence (anyone else here ever cheat on a diet??). But they can give us some direction. For instance, a systematic analysis by Nirgianakis et al. (2021) looked at a few recent studies on diet’s effect on endometriosis symptoms. While, unfortunately, the data was not strong enough for any strong conclusions, it can give some clues for individuals with endometriosis (along with consultation with a healthcare provider).
Two of the diets looked at included the Mediterranean diet and a diet low in fermentable oligo-, di-, monosaccharides, and polyols (FODMAP). Both showed promise for help with endometriosis symptoms, particularly gastrointestinal symptoms and pain.
Nirgianakis et al., (2021) explains:
“FODMAPs are poorly absorbed, short-chain carbohydrates that are readily fermentable by bacteria. Their osmotic actions and gas production may cause intestinal luminal distension inducing pain and bloating in patients with visceral hypersensitivity with secondary effects on gut motility….Diseases like irritable bowel syndrome and endometriosis come along with visceral hypersensitivity, implementing the hypothesis of symptom-reduction after sticking to a low-FODMAP diet. This is very important given the high prevalence of gastrointestinal-related symptoms and co-morbidities in patients with endometriosis. Interestingly, the low-FODMAP diet includes not only a low-Ni diet, but also a low-lactose and a low-gluten diet, thus covering the above-mentioned diets and a large spectrum of high-prevalence pathologies, such as lactose intolerance and non-celiac gluten sensitivity. It is therefore possible to obtain clinical benefits from a low-FODMAP diet, even if at the cost of probably not necessary dietary exclusions.”
The Mediterranean diet includes “fresh vegetables, fruit, white meat, fish rich in fat, soy products, whole meal products, foods rich in magnesium, and cold-pressed oils,” while avoiding “sugary drinks, red meat, sweets, and animal fats”. The review noted that “a significant relief of general pain, dysmenorrhea, dyspareunia, and dyschezia as well as an improvement in the general condition was found.” Moreover, the “Mediterranean diet has well-known antioxidant effects. However, the Mediterranean diet does not involve just the supplementation of certain antioxidants, but rather a collection of eating habits and may thus improve endometriosis-associated pain via additional mechanisms. Fish as well as extra virgin olive oils have been shown to exert anti-inflammatory effects. Specifically, extra virgin olive oil, which contains the substance oleocanthal, displays a similar structure to the molecule ibuprofen, and both take effect via the same mechanism, i.e., cyclooxygenase inhibition. Moreover, the increased amount of fibers provides a eupeptic effect while foods high in magnesium could prevent an increase in the intracellular calcium level and advance the relaxation of the uterus. Taking into account the lack of risks or side effects even after long-term lifetime adherence to this diet and the possible other general health benefits, clinicians may suggest this type of dietary intervention to patients with endometriosis who wish to change their nutritional habits.”
Finally, the authors looked at a qualitative study and found that “the participants experienced an increase in well-being and a decrease in symptoms following their dietary and lifestyle changes. They also felt that the dietary changes led to increased energy levels and a deeper understanding of how they could affect their health by listening to their body’s reactions.” So, taking control of your diet can help improve your general sense of well-being.
Again, there was not strong evidence from any of the studies reviewed, but it might prove helpful when discussing complementary therapies with your healthcare provider. You can find more information about diet and endometriosis here.
Reference
Nirgianakis, K., Egger, K., Kalaitzopoulos, D. R., Lanz, S., Bally, L., & Mueller, M. D. (2021). Effectiveness of Dietary Interventions in the Treatment of Endometriosis: a Systematic Review. Reproductive Sciences, 1-17. Retrieved from https://link.springer.com/article/10.1007/s43032-020-00418-w

Life altering disease and caregivers
Endometriosis can have a profound effect on a person’s ability to work, care for their home, care for their family, and even care for themselves- and this impacts their loved ones as well (Missmer et al., 2021). Endometriosis can have a “negative impact on intimate relationships” (Facchin et al., 2021). It is essential for the person with endometriosis and their support person(s) to have a plan to take care of both of themselves.
The impact endometriosis has on the activities of daily life is not well understood by the general population. This makes it difficult for even loved ones and family members to understand why you may be so fatigued or in too much pain some days to do what you might be able to other days- not to mention the emotional toll it can have. Education for loved ones about the disease itself is important as is education about the treatment. To “minimize the negative impact of endometriosis” on an individual’s life course, “early diagnosis and effective intervention in treating the disease” is imperative (Missmer et al., 2021). This is what we advocate for so strongly- early diagnosis and effective treatment to minimize the impact on a person’s life!
Once your support person or caregiver has a better understanding of the disease and its treatment, you can both develop a plan on how to handle its impact on your lives. Endometriosis can be life altering for those of us with it and those around us. It is important to address the way endometriosis affects our daily lives and have a plan to care for ourselves and our caregivers. This could be parents, partners, children, and various other loved ones involved in our lives. Each might have a different role to play and its good to have a collective plan to lessen the detrimental effects of endometriosis.
For those of us with endometriosis, remember it’s okay to need help. It is easy to feel guilty about not being able to do things, but don’t feel guilty for the effects of a chronic illness. You are doing the best you can. Accept help when it’s offered. Be realistic about what you need to live your best life possible where you are at. Borrowing from the Marine Corps, we have to improvise and adapt if we are to overcome. You are worth the effort.
For the caregivers in our lives- thank you. You’ll never know how much it means to have someone love, understand, and support us on this difficult journey. There are many of us who don’t have that support in our lives and are most acutely aware of how much it would mean. We want you to take care of yourself too. The following is for anyone who is in a caregiver role (including those of us with endometriosis who are in a caregiver role as well):
Being a support person or a caregiver can be both difficult and rewarding. When you start to feel the weight of it, there is a nursing diagnosis for it called “caregiver role strain” (Wayne, 2017). “While caregiving can be rewarding and positive, many family caregivers experience significant physical, psychological, and financial stressors in association with their caregiving role” (Wayne, 2017). This strain can come from multiple factors, such as unrealistic expectations (you won’t be able to fix us), juggling multiple roles (such as income earner, caregiver to other family members), lack of a support system (especially with a disease that others may not understand or may even trivialize), financial pressures, demands of care, social isolation, and neglecting your own well-being (FreedomCare, 2020).
From Wayne (2017), here are some things that might help with reducing caregiver role strain:
- Set aside time for yourself. Take care of your own physical and emotional needs. You can’t pour from an empty cup- you need time to rebuild your physical and emotional energy.
- Utilize stress-reducing methods- “It is important that the caregiver has the opportunity to relax and reenergize emotionally throughout the day to assume care responsibilities.”
- Participate in a support group if there is one available close by or online.
- Discuss problems, concerns, and feelings with a support person or a counselor. Sometimes you need someone outside the family to talk to. Taking on the caregiver role can change dynamics of the relationship and it can take effort to keep the “normal” relationship stuff going.
- Accept help! Ask and allow other available family and friends to assist with caregiving. “Successful caregiving should not be the sole responsibility of one person.”
- Make life chores easy on the both of you. For example, having occasional (or regular if you are able!) housekeeping services or deciding to get takeout food rather than cook one night can help relieve the burden sometimes. It’s okay if it’s not perfect.
Resources:
- Find more at: https://icarebetter.com/learning-library/patient-stories/
- Wondering if you are suffering from caregiver role strain? You can use the Modified Caregiver Strain Index to assess and talk to your healthcare provider about ways to help cope: https://www.sralab.org/sites/default/files/2017-07/issue-14.pdf
- Endowhat: “Caregivers” https://www.endowhat.org/caregivers
References
Facchin, F., Buggio, L., Vercellini, P., Frassineti, A., Beltrami, S., & Saita, E. (2021). Quality of intimate relationships, dyadic coping, and psychological health in women with endometriosis: Results from an online survey. Journal of Psychosomatic Research, 146, 110502. Retrieved from https://doi.org/10.1016/j.jpsychores.2021.110502
FreedomCare. (2020). What is caregiver strain and how to avoid it. Retrieved from https://www.freedomcareny.com/posts/caregiver-role-strain
Missmer, S. A., Tu, F. F., Agarwal, S. K., Chapron, C., Soliman, A. M., Chiuve, S., … & As-Sanie, S. (2021). Impact of endometriosis on life-course potential: a narrative review. International Journal of General Medicine, 14, 9. doi: 10.2147/IJGM.S261139
Wayne, G. (2017). Caregiver role strain nursing care plan. Retrieved from https://nurseslabs.com/caregiver-role-strain/

Insomnia and poor sleep with endometriosis
Sleep quality in individuals with endometriosis is significantly worse than those without it (Nunes et al., 2015). It seems like a no-brainer that pain and other symptoms from endometriosis can affect sleep quality. In fact, pain from endometriosis is known to affect a person’s “work/school, daily activities, exercise, and sleep to a moderate-extreme degree” (DiVasta et al., 2018). And in a vicious cycle, pain affects sleep and poor sleep affects pain. We get how pain can affect sleep, but what are the mechanics behind poor sleep affecting pain?
Ishikura et al. (2020) explains:
“It is well known that any pain condition can affect sleep, leading to sleep disturbances and impairment in sleep quality. In turn, sleep disruption can activate inflammatory mechanisms by triggering changes in the effector systems that regulate the immune system, resulting in abnormal increases in inflammatory responses that can stimulate or increase pain. This can result in the creation of a vicious cycle, with pain causing sleep disturbance that increases inflammation, leading to increased pain. Moreover, experimental studies have shown that the association of sleep loss and inflammatory markers are stronger in females than males, suggesting that women with both insomnia and endometriosis complaints are more susceptible to symptoms of pain. Endometriosis induces several debilitating symptoms that affect women´s lives, including insomnia; however, there have been very few studies of this association…. Treating insomnia would reduce the negative outcomes related to the inflammatory- and pain-related aspects of endometriosis and would contribute to an improvement in mental health and daytime function.”
This poor sleep can increase fatigue, affect quality of life, increase stress, and be detrimental to mental health in those with endometriosis (Arion et al., 2020; Ramin-Wright et al., 2018). Hormonal fluctuations within the menstrual cycle can affect sleep quality as well (drop in progesterone before menses, rise in body temperature during the luteal phase). Some hormonal treatments can affect sleep (Brown et al., 2008).
What can we do to help our sleep? Step one is to have a plan to address the underlying factors affecting sleep such as removing endometriosis. In the meantime, practice pain reduction techniques (nutrition,complimentary therapies such as yoga, pelvic physical therapy, etc.), practice good sleep hygiene, and talk to your healthcare provider about ways to manage pain and insomnia. One study indicated that “melatonin improved sleep quality” and “reduced the risk of using an analgesic by 80%” in patients with endometriosis (Schwertner et al., 2013). The American Academy of Sleep Medicine (2020) reports that cognitive behavioral therapy is the most effective therapy for chronic insomnia. They also suggest:
Keep a consistent sleep schedule. Get up at the same time every day, even on weekends or during vacations.
Set a bedtime that is early enough for you to get at least 7-8 hours of sleep.
Don’t go to bed unless you are sleepy.
If you don’t fall asleep after 20 minutes, get out of bed. Go do a quiet activity without a lot of light exposure. It is especially important to not get on electronics.
Establish a relaxing bedtime routine.
Use your bed only for sleep and sex.
Make your bedroom quiet and relaxing. Keep the room at a comfortable, cool temperature.
Limit exposure to bright light in the evenings.
Turn off electronic devices at least 30 minutes before bedtime.
Don’t eat a large meal before bedtime. If you are hungry at night, eat a light, healthy snack.
Exercise regularly and maintain a healthy diet.
Avoid consuming caffeine in the afternoon or evening.
Avoid consuming alcohol before bedtime.
Reduce your fluid intake before bedtime.
American Academy of Sleep Medicine (2020)
References
American Academy of Sleep Medicine. (2020). Healthy sleep habits. Retrieved from https://sleepeducation.org/healthy-sleep/healthy-sleep-habits/
Arion, K., Orr, N. L., Noga, H., Allaire, C., Williams, C., Bedaiwy, M. A., & Yong, P. J. (2020). A quantitative analysis of sleep quality in women with endometriosis. Journal of Women’s Health, 29(9), 1209-1215. Retrieved from https://www.liebertpub.com/doi/abs/10.1089/jwh.2019.8008
Brown, S. G., Morrison, L. A., Larkspur, L. M., Marsh, A. L., & Nicolaisen, N. (2008). Well-being, sleep, exercise patterns, and the menstrual cycle: a comparison of natural hormones, oral contraceptives and depo-provera. Women & health, 47(1), 105-121. Retrieved from https://doi.org/10.1300/J013v47n01_06
DiVasta, A. D., Vitonis, A. F., Laufer, M. R., & Missmer, S. A. (2018). Spectrum of symptoms in women diagnosed with endometriosis during adolescence vs adulthood. American journal of obstetrics and gynecology, 218(3), 324-e1. Retrieved from https://doi.org/10.1016/j.ajog.2017.12.007
Ishikura, I. A., Hachul, H., Pires, G. N., Tufik, S., & Andersen, M. L. (2020). The relationship between insomnia and endometriosis. Journal of Clinical Sleep Medicine, 16(8), 1387-1388. Retrieved from https://doi.org/10.5664/jcsm.8464
Nunes, F. R., Ferreira, J. M., & Bahamondes, L. (2015). Pain threshold and sleep quality in women with endometriosis. European Journal of Pain, 19(1), 15-20. Retrieved from https://doi.org/10.1002/ejp.514
Ramin-Wright, A., Schwartz, A. S. K., Geraedts, K., Rauchfuss, M., Wölfler, M. M., Haeberlin, F., … & Leeners, B. (2018). Fatigue–a symptom in endometriosis. Human reproduction, 33(8), 1459-1465. Retrieved from https://doi.org/10.1093/humrep/dey115
Schwertner, A., Dos Santos, C. C. C., Costa, G. D., Deitos, A., de Souza, A., de Souza, I. C. C., … & Caumo, W. (2013). Efficacy of melatonin in the treatment of endometriosis: a phase II, randomized, double-blind, placebo-controlled trial. PAIN®, 154(6), 874-881. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S030439591300081X

What’s all the buzz about the bowel?
The bloating, cramping, diarrhea, constipation, pain with bowel movements, nausea…could this be endometriosis?
Yes, it could.
Irritable bowel syndrome (IBS) like symptoms are common with endometriosis- up to 85% of endometriosis patients have gastrointestinal/bowel symptoms (Aragon & Lessey, 2017; Ek et al., 2015). It can be difficult to distinguish if it is endometriosis causing the IBS-like symptoms or if IBS is occurring along with endometriosis. Ek (2019) noted that “several potential shared pathophysiological mechanisms exist between endometriosis and IBS, such as chronic low-grade inflammation, increased mast cell numbers, increased mast cell activation, visceral hypersensitivity, altered gut microbiota and increased intestinal permeability, which has been described in relation to both endometriosis and IBS.” IBS symptoms can be helped with a low FODMAPs diet, and studies have noted that those with both IBS type symptoms AND endometriosis found improvement with a low FODMAPs diet (Moore et al., 2017). (See more info on bowel/GI endometriosis)
Endometriosis does not have to be on the bowel to cause bowel symptoms. Most of the time, symptoms may be due to irritation from lesions near the bowel (such as posterior cul de sac, Pouch of Douglas, uterosacral ligaments, etc.) or from adhesions pulling on the bowel (Aragon & Lessey, 2017; Ek et al., 2015). The incidence of endometriosis on the bowel itself ranges from 5% to 12% of those with endometriosis (Habib et al., 2020).
When endometriosis does involve the bowel, it most often found on the sigmoid colon, “followed by the rectum, ileum, appendix, and caecum” (Charatsi et al., 2018). “Extremely rare locations that have been reported include the gallbladder, the Meckel diverticulum, stomach, and endometriotic cysts of the pancreas and liver” (Charatsi et al., 2018). It can be difficult to determine bowel involvement from symptoms alone. Symptoms can range from none to crampy abdominal pain, constipation, diarrhea, pain with bowel movements, nausea, vomiting, and rarely rectal bleeding (Charatsi et al., 2018). Symptoms may be acyclical (all month long) and then aggravated during your period (Charatsi et al., 2018).
If your surgeon is suspicious of bowel involvement, they may do imaging prior to surgery to help guide care. Transvaginal ultrasounds and magnetic resonance imaging (MRIs) can be useful in detecting bowel involvement (but don’t necessarily rule it out) (Guerriero et al., 2018). According to one center that specializes in endometriosis surgery, “lesions on the colon, especially the distal sigmoid and rectum, I find ultrasound to be the most reliable” with the limitation that “it will only image the distal 20 cm of the colon, and lesions above that will be missed” (Pacific Endometriosis and Pelvic Surgery, n.d.). “For higher lesions on the sigmoid, the right colon, and small bowel then MRI is more accurate” (Pacific Endometriosis and Pelvic Surgery, n.d.).
Will surgery fix those IBS-like symptoms? It can be difficult to find studies that prove that. Mostly because “surgical techniques are not standardized” (Wolthuis et al., 2014). However, one center that specializes in endometriosis surgery found (with questionnaires of their patients) that their patients saw an “80% reduction in most bowel symptoms” (Center for Endometriosis Care, 2020). This rate may not be found with general gynecology surgery. If you think you might have bowel involvement, it is important to find the right care. The success of surgery depends on the skills and experience of the surgeon and a multidisciplinary team. It is recommended that “surgery should be performed by experienced surgeons, in centres with access to multidisciplinary care” (Habib et al., 2020, para. 1). While hormonal medications have been shown to help relieve symptoms, it may not stop the progression of the disease which can lead, in severe cases, to bowel obstruction; therefore, it is recommended that close follow-up be utilized if you do not choose surgical treatment (Habib et al., 2020; Ferrero et al., 2011).
- Interested in more info on bowel endo care from the experts? See the Endo Summit’s videos found on YouTube: https://www.youtube.com/watch?v=QJRkk4-6cSk and https://www.youtube.com/watch?v=BXUllhdW2h0
- For more on surgical technique for bowel endometriosis look here.
- You can search for surgeons with skill on bowel endometriosis here.
- Problems with pelvic floor dysfunction and other issues can also contribute to some symptoms- see Pelvic Floor Dysfunction
References
Aragon, M., & Lessey, B. A. (2017). Irritable Bowel Syndrome and Endometriosis: Twins in Disguise. GHS Proc, 43-50. Retrieved from https://hsc.ghs.org/wp-content/uploads/2016/11/GHS-Proc-Ibs-And-Endometriosis.pdf
Center for Endometriosis Care. (2020). Bowel endometriosis. Retrieved from https://centerforendo.com/endometriosis-and-bowel-symptoms
Charatsi, D., Koukoura, O., Ntavela, I. G., Chintziou, F., Gkorila, G., Tsagkoulis, M., … & Daponte, A. (2018). Gastrointestinal and urinary tract endometriosis: a review on the commonest locations of extrapelvic endometriosis. Advances in medicine, 2018. Retrieved from https://doi.org/10.1155/2018/3461209
Ek, M. (2019). Gastrointestinal symptoms in women with endometriosis. Aspects of comorbidity, autoimmunity and inflammatory mechanisms (Doctoral dissertation, Lund University).
Ek, M., Roth, B., Ekström, P., Valentin, L., Bengtsson, M., & Ohlsson, B. (2015). Gastrointestinal symptoms among endometriosis patients—A case-cohort study. BMC women’s health, 15(1), 59. doi: 10.1186/s12905-015-0213-2
Ferrero, S., Camerini, G., Maggiore, U. L. R., Venturini, P. L., Biscaldi, E., & Remorgida, V. (2011). Bowel endometriosis: Recent insights and unsolved problems. World journal of gastrointestinal surgery, 3(3), 31. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3069336/
Guerriero, S., Saba, L., Pascual, M. A., Ajossa, S., Rodriguez, I., Mais, V., & Alcazar, J. L. (2018). Transvaginal ultrasound vs magnetic resonance imaging for diagnosing deep infiltrating endometriosis: systematic review and meta‐analysis. Ultrasound in Obstetrics & Gynecology, 51(5), 586-595. Retrieved from https://obgyn.onlinelibrary.wiley.com/doi/full/10.1002/uog.18961
Habib, N., Centini, G., Lazzeri, L., Amoruso, N., El Khoury, L., Zupi, E., & Afors, K. (2020). Bowel Endometriosis: Current Perspectives on Diagnosis and Treatment. International Journal of Women’s Health, 12, 35. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6996110/
Moore, J. S., Gibson, P. R., Perry, R. E., & Burgell, R. E. (2017). Endometriosis in patients with irritable bowel syndrome: specific symptomatic and demographic profile, and response to the low FODMAP diet. Australian and New Zealand Journal of Obstetrics and Gynaecology, 57(2), 201-205. Retrieved from https://doi.org/10.1111/ajo.12594
Pacific Endometriosis and Pelvic Surgery. (n.d.) Bowel disease. Retrieved from https://pacificendometriosis.com/bowel-disease/?fbclid=IwAR1EVUZJHHVk7wvdGwTwJ6Mo8QICiY8ktRtCXIotvhQzKqvTqa0LSjEZs-k
Wolthuis, A. M., Meuleman, C., Tomassetti, C., D’Hooghe, T., van Overstraeten, A. D. B., & D’Hoore, A. (2014). Bowel endometriosis: colorectal surgeon’s perspective in a multidisciplinary surgical team. World Journal of Gastroenterology: WJG, 20(42), 15616. doi: 10.3748/wjg.v20.i42.15616

Mast cells and endometriosis
Endometriosis is an inflammatory disorder, and this inflammation can lead to increased pain, fatigue, and general feelings of unwellness. Mast cells are immune system cells that can stimulate inflammation (Graziottin, Skaper, & Fusco, 2014). Mast cells hold proinflammatory substances (such as histamine, cytokines, prostaglandins, and more), and, when activated, release these proinflammatory substances (Weller, n.d.). When responding to a threat to the body and for healing, this is a good thing. But when mast cells are activated in endometriosis, not so much.
Activated mast cells (the ones that have released all those proinflammatory substances) have been found in higher quantities in endometriosis lesions versus normal tissue (Hart, 2015; Indraccolo & Barbieri, 2010; Sugamata et al., 2005). Estrogen seems to stimulate mast cells to support the inflammatory process (Zhu et al., 2018). In fact, estrogen receptors are found on mast cells and the high local levels of estrogen from endometriotic lesions may activate the mast cells and lead to pain (Hart, 2015; Zhu et al., 2018). While many therapies for endometriosis involve lowering estrogen production by the feedback loop between the brain and the ovaries, it should be remembered that endometriosis lesions demonstrate production of estrogen themselves (and also show resistance to progesterone) (Delvoux et al., 2009). In fact, the level of estrogen in endometriosis lesions were related to pain symptoms in patients with endometriosis while blood levels of estrogen were not (Zhu et al., 2018).
In addition, nerve fibers in endometriosis lesions have been shown to “release neural peptides such as nerve growth factor and substance P” that in turn activate mast cells to release those proinflammatory substances “which contributes to the development of pain and hyperalgesia in patients with endometriosis” (Zhu & Zhang, 2013). Those granules released by mast cells can contribute to new blood vessel growth, more inflammation, and nerve growth, which can lead to pain (Graziottin, 2009). This persistent inflammation from endometriosis lesions “intensifies neurogenic inflammation and tissue damage” leading to “progressive functional and anatomic damage associated with prominent tissue scarring, exemplified by the natural history of endometriosis” and “up-regulation of nerve pain” (Graziottin, 2009).
So, mast cells are recruited to endometriosis lesions, respond to the higher local estrogen and other inflammatory conditions, release their proinflammatory substances which can lead to pain and scarring. This effect of mast cells is associated in other pain syndromes as well, such as interstitial cystitis, IBS, vulvodynia, complex regional pain syndrome, migraines, and fibromyalgia (Aich et al., 2015).
References
Aich, A., Afrin, L. B., & Gupta, K. (2015). Mast cell-mediated mechanisms of nociception. International journal of molecular sciences, 16(12), 29069-29092. Retrieved from https://doi.org/10.3390/ijms161226151
Delvoux, B., Groothuis, P., D’Hooghe, T., Kyama, C., Dunselman, G., & Romano, A. (2009). Increased production of 17β-estradiol in endometriosis lesions is the result of impaired metabolism. The Journal of Clinical Endocrinology & Metabolism, 94(3), 876-883. Retrieved from https://academic.oup.com/jcem/article/94/3/876/2596530
Graziottin, A., Skaper, S. D., & Fusco, M. (2014). Mast cells in chronic inflammation, pelvic pain and depression in women. Gynecological Endocrinology, 30(7), 472-477. Retrieved from https://www.tandfonline.com/doi/abs/10.3109/09513590.2014.911280
Graziottin, A. (2009). Mast cells and their role in sexual pain disorders. Female Sexual Pain Disorders, 176. Retrieved from https://www.fondazionegraziottin.org/ew/ew_articolo/1820%20-%20mast%20cells%20and%20SPD.pdf
Hart, D. A. (2015). Curbing inflammation in multiple sclerosis and endometriosis: should mast cells be targeted?. International journal of inflammation, 2015. Retrieved from https://www.hindawi.com/journals/iji/2015/452095/
Indraccolo, U., & Barbieri, F. (2010). Effect of palmitoylethanolamide–polydatin combination on chronic pelvic pain associated with endometriosis: Preliminary observations. European Journal of Obstetrics & Gynecology and Reproductive Biology, 150(1), 76-79. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0301211510000424
Sugamata, M., Ihara, T., & Uchiide, I. (2005). Increase of activated mast cells in human endometriosis. American journal of reproductive immunology, 53(3), 120-125. Retrieved from https://doi.org/10.1111/j.1600-0897.2005.00254.x
Weller, C. (n.d.). Mast cells. Retrieved from https://www.immunology.org/public-information/bitesized-immunology/cells/mast-cells
Zhu, T. H., Ding, S. J., Li, T. T., Zhu, L. B., Huang, X. F., & Zhang, X. M. (2018). Estrogen is an important mediator of mast cell activation in ovarian endometriomas. Reproduction, 155(1), 73-83. Retrieved from https://doi.org/10.1530/REP-17-0457
Zhu, L., & Zhang, X. (2013). Research advances on the role of mast cells in pelvic pain of endometriosis. Journal of Zhejiang University (Medical Science), 42(4), 461. DOI: 10.3785/j.issn.1008-9292.2013.04.015

FAQ’s, Podcasts, Resources About Endo, and More!
You can find a diverse gathering of information about endometriosis on our website. We have some information you may not have thought to look for or were unsure of where it might located. Here’s a glimpse at a few of the resources you can find:
In our Resources section, you will find material that includes a wide variety of topics and links to help you on your endometriosis journey.
- If you prefer to listen instead of read, we have several links to podcasts, videos, and webinars.
- If you are looking for info on advocacy and other helpful sources, then see here.
- Need information about navigating insurance? We have info on what to know to help be your own best advocate- as well as info for those on Tricare
- We have topics specific for teens, infertility, pregnancy, and LGBTQIA+
- Tips for topics such as keeping track of your personal medical history, things to pack for surgery/hospital, what to expect before and after surgery, and more.
- Resources for those in the UK and Australia
- and more!
In our Frequently Asked Questions section, you can find answers to questions such as:
- Is that really true? Info on Myths and Misinformation
- Is endometriosis an autoimmune disease?
- Does endometriosis increase my risk of cancer?
- Is There Microscopic or Occult Endometriosis
- Can endometriosis persist after hysterectomy/ovary removal/menopause?
- Is there a genetic component to endometriosis?
- Is there a link between heart disease and endometriosis?
- What effects can long term low estrogen cause?
Endometriosis has several related conditions that can cause similar symptoms. While treating endometriosis is important, it is equally important to treat these other conditions that might be present in order to find relief.
- Adenomyosis
- Endometrial/Uterine Polyps
- Interstitial Cystitis/Bladder Pain Syndrome
- Pelvic Floor Dysfunction
- Fibroids (Leiomyomas)
- Polycystic Ovarian Syndrome (PCOS)
- Pudendal Neuralgia and Vulvodynia
- Pelvic Congestion Syndrome
- Occult Hernia
- Migraines and Endometriosis
Information about endometriosis itself and its treatment can be found throughout the website.
- What makes endometriosis different from the lining of the uterus? Differences in how endometriosis looks and behaves (how it behaves in response to estrogen and progesterone, can make its own nerves and blood vessels, as well as other differences)
- Where can endometriosis be found in the body? (including some weird places)
- How does endometriosis start?
- What are the symptoms of endometriosis?
- How is it diagnosed? How useful are an ultrasound, MRI, or labwork with endometriosis?
- Why is excision surgery recommended? Why should I see a specialist?
- What treatment options are there?
You’ll find all these topics and more on the website. Start exploring!

Your Story Isn’t Over; Mental Health Awareness
May is mental health awareness month and a good time to shine a light on the affects that endometriosis has on our mental health. A significant number of people worldwide suffer from a mental health disorder. While mental health covers a wide spectrum of disorders, two of the most pervasive are anxiety and depression (NAMI, 2021). Both of these not only affect a large portion of the population in general, but also can be found in higher rates in those with chronic illnesses- especially those involving chronic pain (Li et al., 2018).
Endometriosis has been associated “a wide spectrum of different types of pain, ranging from severe dysmenorrhea to chronic pelvic and other comorbid pain conditions” and those with endometriosis have an “elevated likelihood of developing depression and anxiety disorders” (Li et al., 2018). Endometriosis greatly affects quality of life, relationships, stress, professional life, and many other factors that can play into depression and anxiety (Donatti et al., 2017; Lagana et al., 2017). While these factors can play into depression and anxiety, research has suggested that endometriosis leads to specific changes in the brain that are associated with pain, anxiety, and depression (Lima Filho et al., 2019). For example, in a study done on mice, researchers found that “endometriosis led to changes in expression of several genes in the brain regions associated with pain, anxiety, and depression” (Li et al., 2018). In addition, some studies have shown a shared genetic predisposition between depression and endometriosis (Adewuyi et al., 2021).
Our mental health is important. As chronic pelvic pain from endometriosis can affect our mental health, it is important to address the underlying cause (Van den Broeck et al., 2013). But we also need to seek care for our mental health in other ways as well. We can’t do it all alone and seeking help from a professional for our mental health is every bit as important as seeking help for a broken bone. Just as we do physical therapy to help our musculoskeletal system, counseling and cognitive behavioral therapy is like physical therapy for our mental well-being. Endometriosis impacts our relationships, our ability to work, our sense of self, and pretty much every aspect of our lives. Seeking help to cope is not a sign of weakness, but of strength. One of my favorite symbols for mental health is from The Semicolon Project. The semicolon is a sign that the sentence, the story, isn’t over yet. Know that you are not alone, and your story isn’t over yet.
National Suicide Prevention Hotline: 1-800-273-8255
References
Adewuyi, E. O., Mehta, D., Sapkota, Y., Auta, A., Yoshihara, K., Nyegaard, M., … & Nyholt, D. R. (2021). Genetic analysis of endometriosis and depression identifies shared loci and implicates causal links with gastric mucosa abnormality. Human Genetics, 140(3), 529-552. doi: 10.1007/s00439-020-02223-6
Donatti, L., Ramos, D. G., Andres, M. D. P., Passman, L. J., & Podgaec, S. (2017). Patients with endometriosis using positive coping strategies have less depression, stress and pelvic pain. Einstein (São Paulo), 15(1), 65-70. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5433310/
Laganà, A. S., La Rosa, V. L., Rapisarda, A. M. C., Valenti, G., Sapia, F., Chiofalo, B., … & Vitale, S. G. (2017). Anxiety and depression in patients with endometriosis: impact and management challenges. International journal of women’s health, 9, 323. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5440042/
Li, T., Mamillapalli, R., Ding, S., Chang, H., Liu, Z. W., Gao, X. B., & Taylor, H. S. (2018). Endometriosis alters brain electrophysiology, gene expression and increases pain sensitization, anxiety, and depression in female mice. Biology of reproduction, 99(2), 349-359. Retrieved from https://doi.org/10.1093/biolre/ioy035
Lima Filho, P. W. L., Chaves Filho, A. J. M., Vieira, C. F. X., de Queiroz Oliveira, T., Soares, M. V. R., Jucá, P. M., … & das Chagas Medeiros, F. (2019). Peritoneal endometriosis induces time-related depressive-and anxiety-like alterations in female rats: involvement of hippocampal pro-oxidative and BDNF alterations. Metabolic brain disease, 34(3), 909-925. Retrieved from https://doi.org/10.1007/s11011-019-00397-1
National Alliance on Mental Illness (NAMI). (2021). Mental health by the numbers. Retrieved from https://www.nami.org/mhstats
Van den Broeck, U., Meuleman, C., Tomassetti, C., D’Hoore, A., Wolthuis, A., Van Cleynenbreugel, B., … & D’Hooghe, T. (2013). Effect of laparoscopic surgery for moderate and severe endometriosis on depression, relationship satisfaction and sexual functioning: comparison of patients with and without bowel resection. Human Reproduction, 28(9), 2389-2397. Retrieved from https://doi.org/10.1093/humrep/det260
